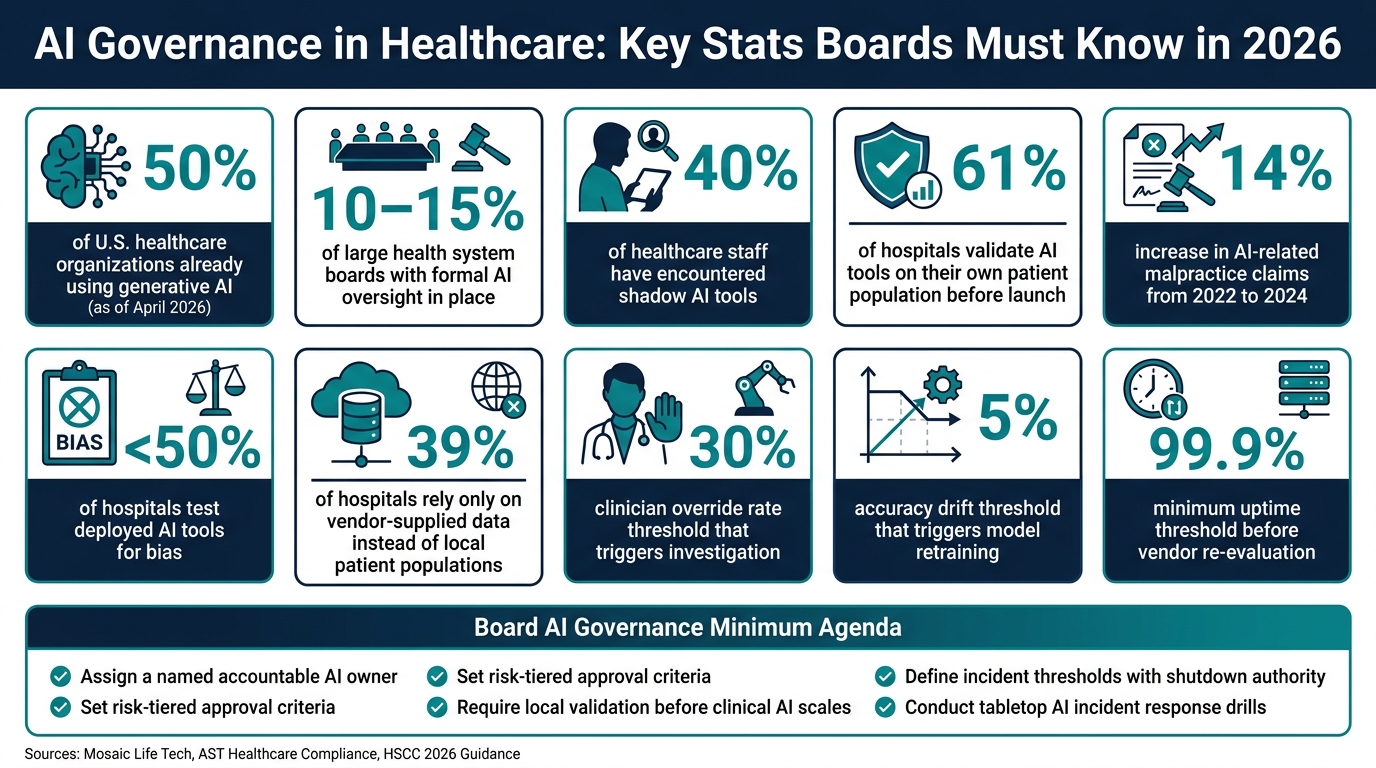
If I were briefing a healthcare board on this article, I’d put the answer first: boards need named AI owners, local testing, PHI controls, vendor checks, and shut-off rules before AI spreads any further. That’s because 50% of surveyed U.S. healthcare organizations had already put generative AI into use by April 2026, while only 10%–15% of large health system boards had formal AI oversight in place. At the same time, 40% of healthcare staff have run into shadow AI tools.
Here’s the article in plain English:
- AI use is no longer a side project. It now touches care, billing, and documentation.
- The board is on the hook for oversight. This now sits with fiduciary duty and documented board review.
- Every AI tool needs one accountable executive. If no one can stop it, no one owns the risk.
- FDA clearance or vendor claims are not enough. Hospitals still need to test tools on their own patients and workflows.
- PHI controls must be provable. Boards need data-flow maps, AI-specific BAAs, and audit logs.
- Vendor risk is still your risk. Third-party models, subprocessors, bias, and silent model updates all need review.
- Incident response must be set before scale. Boards should know who can pause a tool, what triggers that step, and how fast it can happen.
A few numbers make the point even sharper:
- 61% of hospitals validate AI tools on their own patient population before launch
- AI-related malpractice claims went up 14% from 2022 to 2024
- Fewer than half of hospitals test deployed AI tools for bias
AI Governance in Healthcare: Key Stats Boards Must Know in 2026
Healthcare AI Governance - Risks, Compliance, and Frameworks Explained
sbb-itb-535baee
Quick overview
| Board question | What I’d want management to show |
|---|---|
| Who owns each AI tool? | Named executive, committee role, escalation path |
| Is the tool safe? | Local validation, override process, rollback plan, drift and bias checks |
| Is PHI handled lawfully? | TPO/authorization path, data maps, BAA terms, logs |
| Are third-party AI vendors under control? | Security review, subprocessor list, update notice, local testing |
| Can we stop a bad tool fast? | Incident rules, shutdown authority, thresholds, drill results |
The core message is simple: this is not about whether AI is useful. It’s about whether the board can see it, govern it, and stop harm before it spreads.
1. Who Is Accountable for AI Decisions, and How Should the Board Oversee Them?
Start with accountability. Every AI system needs one named executive who answers for it. Committees can review the work, but an owner has to own the outcome.
"If the answer to 'who explains and stops this if the tool causes harm?' is 'the committee,' that's a governance gap, not a governance structure." - Mosaic Life Tech [2]
Boards should require a named executive accountable for every AI system. That person needs the authority to pause or stop a deployment when safety concerns show up. The same owner should control approval, monitoring, and decommissioning. Alongside that person, a cross-functional group should have clear roles across clinical, compliance, cybersecurity, privacy, legal, and operations. If the board can't name the owner, it can't govern the tool.
Questions Boards Should Ask About Ownership and Committee Structure
The starting point is simple: management should be able to answer a few direct questions on the spot.
- Who is the named executive accountable for AI governance, and do they have authority to pause or stop a deployment?
- Which committee - Audit, Quality, or another - formally owns AI oversight, and is that written into its charter?
- When does an AI issue move from a committee to the full board? What triggers that escalation?
- How are responsibilities split across clinical, compliance, cybersecurity, privacy, and legal leaders?
Role clarity matters here. Clinical leaders validate tools against the organization's patient data and workflows. The CIO/CTO own inventory and controls. Legal and compliance own regulatory risk. Cybersecurity and privacy own PHI, access, drift, and shadow AI. Operations own workflow impact.
What Board Reporting on AI Should Include
Board reporting on AI should be an auditable dashboard, not a loose narrative update. Directors need a clear, data-based view of what's in use, what's at risk, and where a decision is needed. At a minimum, quarterly reports should cover:
| Reporting Element | Why It Matters |
|---|---|
| Total AI systems in use, classified by risk level | Establishes the full scope of exposure |
| High-risk use cases awaiting or under review | Flags where approval decisions are pending |
| Validation status for high-impact tools | Shows whether local testing is complete |
| Unresolved control gaps or failed validation checks | Surfaces where governance has broken down |
| Open vendor issues or contract concerns | Tracks third-party accountability |
| AI incidents, near-misses, and bias findings | Provides early warning before harm occurs |
That dashboard gives the board the base it needs for the next issue: whether the tool is safe, clinically valid, and stable over time.
2. How Should Boards Evaluate Patient Safety, Clinical Quality, and Model Performance?
Once ownership is clear, the next job is simple to state and hard to do: prove the tool is safe before it goes live.
Boards should require proof of validation, monitoring, and rollback controls before any clinical AI tool used for diagnosis, triage, decision support, or documentation is deployed. In practice, that means testing three things: clinical safety, fit with day-to-day workflows, and performance after launch.
Only 61% of hospitals validate AI tools on their own patient population before deployment. And FDA clearance is not enough on its own. A hospital still needs to test the tool on its own patients and workflows. If the tool touches the medical record, the next issue is data compliance.
Questions to Ask Before Approving a Clinical or Documentation AI Tool
Before any clinical AI tool goes live, management should be able to answer these questions plainly:
- Was this tool validated on our patient population, or only on vendor-supplied data?
- How do clinicians override the output?
- How are hallucinations caught before notes reach the medical record?
- What is the rollback plan if performance drops in production?
- Has the tool been tested for bias across demographic groups?
Pieces Technologies is a good reminder that vendor accuracy claims need to be checked, not taken at face value. In May 2024, the Texas Attorney General reached a settlement with Pieces Technologies over allegations that the company made misleading claims about the accuracy of its generative AI tools used for clinical summaries in hospitals [2][3].
"If you cannot answer what the model saw, what the model returned, and whether a human overrode it, you cannot defend it." - Nadeem Khadim, Healthcare Compliance, AST [4]
For high-risk decisions, human review is not optional. CMS regulations require that any AI-driven adverse coverage determination in Medicare Advantage be reviewed by a licensed physician before it is issued [1]. Boards should treat that as the floor for any AI tool that shapes patient care decisions.
Safety and Quality Metrics the Board Should See
After approval, boards need production metrics, not just pre-launch promises. These metrics should be reviewed on a fixed schedule, with clear escalation when thresholds are crossed.
| Metric | Meaning | Threshold for Action |
|---|---|---|
| Clinician override rate | How often staff reject AI recommendations | Investigate if override rate exceeds 30% [2][4] |
| Note correction rate | Frequency of edits to AI-generated clinical notes | Retrain or review if corrections trend upward [4] |
| Near-misses and adverse events | Direct patient safety signals | Immediate escalation on any adverse event [2][4] |
| Drift from baseline | Performance deviation from baseline after deployment | Retrain if accuracy drifts more than 5% from baseline [4] |
| Workflow uptime | Operational reliability of critical tools | Re-evaluate vendor if uptime falls below 99.9% [4] |
| Bias monitoring results | Disparate outcomes across demographic groups | Escalate if demographic disparities emerge [2][4] |
One metric deserves extra attention: a zero override rate is not always good news. It can point to automation bias rather than trust earned through good performance. AI-related malpractice claims increased 14% between 2022 and 2024, with automation bias cited as a leading factor [2].
"No reported incidents may mean monitoring is weak, not that the tool is safe." - Teresa Younkin, CEO, Mosaic Life Tech [2]
Safety findings should then feed into the next governance issue: whether the data, training set, and AI use comply with the rules.
3. Are HIPAA, Data Use, and AI Compliance Controls Actually in Place?
A tool can help in a clinical setting and still mishandle PHI. Once an AI tool is live, a board needs more than verbal comfort. It needs documented proof that data moving through the tool is handled lawfully. That puts the focus on two things: data-flow control and contract terms.
"AI compliance is not static; it is a living and evolving risk environment." - Morgan Lewis [5]
Questions Boards Should Ask About PHI, Training Data, and Generative AI Use
The biggest question sounds simple: does the organization have a permitted HIPAA pathway for each data flow?
Under HIPAA, management should be able to point to a specific path for the data before it enters the model. That usually means Treatment, Payment, or Healthcare Operations (TPO). If TPO does not apply, management should be able to show valid patient authorization. If neither exists, the data must be de-identified to HIPAA standards before use.
That is why boards should ask management to name the pathway for each active AI tool. A broad answer like “it’s covered by HIPAA” isn’t enough.
Generative AI adds another risk layer. Staff can paste PHI into tools that were never approved in the first place. Boards should ask how those tools are detected, blocked, and reported.
AI-specific BAAs should spell out where PHI goes, bar model training on patient data, and address cloud environments. Boards should also check whether vendor claims about de-identification are tested, not just taken at face value [5]. Once the data path is clear, the board can judge whether the vendor’s controls fit the level of risk.
Evidence Boards Should Be Able to Review
If management cannot produce these items when asked, the controls are not in place in any meaningful sense. They are goals, not proof.
| Artifact | What It Proves |
|---|---|
| PHI-touching AI tools and data paths | All PHI-touching tools are known, grouped by risk level, with documented data flows that include external vendor environments [2][3][5] |
| Data flow maps | The exact path PHI takes, including external vendor environments and generative AI prompts [1][5] |
| AI-specific BAAs | Vendor contracts that limit model training rights, define data retention, and address cloud environments [5] |
| Privacy and security assessments | Review happened before deployment, not only after a problem appears |
| Audit logs | Technical proof that AI access and outputs can be reviewed and traced [4][5] |
"If you cannot trace a prediction back to a versioned model, dataset, and approver, you do not have governance - you have a memo." - Nadeem Khadim, Healthcare Compliance, AST [4]
That kind of traceability is where vendor oversight and incident response start.
4. How Should Boards Govern Third-Party AI Vendors, Cybersecurity Risk, and Model Bias?
Once PHI flows are mapped, the next question is simple: who controls the vendor handling that data?
PHI is already tough to track inside a health system. Once it moves through a vendor’s model and its subprocessors, it gets even harder to follow. But one thing does not change: the organization still owns the accountability. That stays true even when the model sits outside the health system. A vendor contract doesn’t make that duty disappear. In 2024, the Texas Attorney General reached a settlement with Pieces Technologies, Inc. over the accuracy and oversight of AI-generated clinical summaries, a reminder that organizations can still be held to account for harmful third-party outputs [2].
There’s also a clear risk signal in the numbers. AI-related malpractice claims rose 14% between 2022 and 2024, while bias testing still varies a lot across hospitals. Fewer than half of hospitals test deployed AI tools for bias, and 39% still rely only on vendor-supplied data instead of checking tools against their own patient populations [2]. That’s a problem. If an external AI tool hasn’t gone through local validation, bias review, and dashboard reporting, the board can’t treat it as governed.
Questions to Ask When Reviewing an External Vendor Model
Before a board approves any external AI tool, management should be ready with direct answers - and the paperwork to back them up.
Start with security and integration. How does the tool connect to the EHR? What level of access does it need? Which subprocessors touch the data? The board should also know whether a cybersecurity review has been completed and whether the vendor has a written incident notification timeline for model drift, security breaches, or performance failures.
Then look at downstream vendor exposure. Are subprocessor relationships documented? Are they covered in the contract and the BAA? HSCC guidance released in April 2026 points to training data leakage as a hidden supply chain risk that many organizations still miss [6].
Next comes model performance and bias. Has the tool been tested on this organization’s patient population, not just the vendor’s benchmark set? Has it been checked for uneven outcomes across patient groups in this system, especially if it affects coverage decisions, clinical triage, or workforce actions? That’s where a lot of risk hides in plain sight.
And don’t skip updates and rollback. Vendors change models. Sometimes quietly. The board needs to know what notice the vendor gives, what testing happens before an update is accepted, and what rollback steps apply if the update causes harm or weakens performance.
Risk Tools and Checklists That Make Vendor Oversight Actionable
These answers shouldn’t live in scattered emails or meeting notes. They belong in two working documents the board can review: a vendor assessment checklist and a living AI risk register.
A vendor AI assessment checklist gives management a repeatable way to review each new tool before it goes live. An AI risk register gives the board a live record of every active tool, including its intended use, data sources, validation status, open findings, and review dates.
| Register Element | What It Tracks |
|---|---|
| Tool inventory | Name, version, risk classification, and authorization log |
| Data governance | PHI storage locations, subprocessor map, and data flow diagrams |
| Performance evidence | Local validation results, bias assessment, and drift monitoring logs |
| Operational controls | Rollback plan, clinician override records, and incident response triggers |
| Contract controls | AI-specific BAA clauses, insurance riders, and vendor security posture |
At a minimum, the board should be able to show three things: the vendor was vetted, the data paths are known, and a rollback plan is ready if the tool harms patients or disrupts operations. Those are the controls that mark the point where a tool should be paused or removed.
5. What Incident Response Plans, Risk Thresholds, and Approval Rules Must Be In Place Before AI Scales?
A risk register only goes so far. The board also needs a clear plan for what happens when an AI system goes off track.
Once AI gets approved, the next board-level job is simple: know how fast it can be paused or shut down.
Questions Boards Should Ask About AI Incident Response and Escalation
AI incidents should be defined before rollout, not after something breaks. That includes drift, bias, unsafe outputs, data leakage, prompt injection, and automation bias. Each one needs a clear response path with a specific owner.
That still isn't enough on its own. A definition on paper doesn't help if no one can act. Boards should require:
- a named executive with shutdown authority
- set performance thresholds
- tabletop response drills that have already been tested
- an anonymous AI safety reporting channel
Response rules also need to match the level of risk before any tool scales. This is where approval rules stop being abstract policy and become a real stop/go control.
Before scaling, management should document the tool's intended use, data provenance, local validation, monitoring plan, rollback process, and named owner. High-risk clinical tools - such as diagnosis, triage, or coverage decisions - need board or committee approval, continuous monitoring, and re-approval after any model, prompt, data, or workflow change.
| Risk Category | Approval | Review Cadence | Reapproval Trigger |
|---|---|---|---|
| Low-risk administrative (e.g., coding, scheduling) | Department/IT | Annual | Major version change |
| Clinical support (e.g., documentation, triage) | Quality Committee | Quarterly | Data source or workflow change |
| High-risk clinical (e.g., diagnosis, autonomous decisioning) | Full board or board committee | Continuous / Monthly | Performance drift, bias, or model update |
Quarterly board reports should show incidents, near-misses, bias results, threshold breaches, remediation progress, and re-approval status. Boards shouldn't settle for a polished dashboard. They should expect a plain answer to one hard question: Are these tools performing safely on this organization's patients?
Conclusion: The Minimum AI Governance Agenda Healthcare Boards Should Act on Now
These governance choices are not optional extras. They're the baseline.
Boards that haven't acted on them are taking on avoidable risk. AI-related malpractice claims rose 14% between 2022 and 2024, fewer than half of hospitals test deployed AI tools for bias, and only 10–15% of large health system boards have formal AI oversight structures in place as of early 2026 [2].
The minimum agenda is concrete:
- assign a named accountable owner for AI governance
- set approval criteria tied to risk level
- require local validation before any clinical tool scales
- define incident thresholds that give someone the authority to shut a tool off
These are governance decisions. They belong at the board level, not buried inside a technical team.
Boards that move now will be in a better position to protect patients and make AI work as intended. The ones that wait are taking on risk they haven't measured and can't yet manage.
FAQs
How should boards prioritize AI risks first?
Boards need to begin with a full inventory of every AI tool used across the organization. If they don’t know what’s in use, who’s using it, or why, they can’t oversee risk in a serious way or spot shadow AI.
From there, management should sort risks by use case, model type, and possible effect on patient care or day-to-day operations. That helps teams focus first on the areas with the most exposure.
What makes an AI tool high risk in healthcare?
An AI tool is high risk in healthcare when it can materially affect patient care, day-to-day clinical work, or regulatory compliance.
That usually includes tools used for diagnosis, triage, clinical ordering, or automated care denials.
Risk goes up fast when a tool does any of the following:
- Produces probabilistic outputs that can sway clinical decisions
- Takes clinical actions automatically
- Introduces bias
- Puts patient privacy at risk
- Lacks local validation on the organization’s own patient data
In plain English: if the tool can shape care, deny care, or create compliance trouble, it belongs in the high-risk category.
How often should boards review AI governance?
Boards need a steady reporting cadence for AI governance if they want to meet their fiduciary duties. A fixed meeting schedule helps, but it shouldn't be the only trigger for oversight.
A better approach is to tie board review to an AI risk register that includes review dates for specific use cases. That way, oversight happens when it should - not just when the calendar says so.
The right frequency depends on the organization's committee structure. It should also support ongoing monitoring of AI performance, safety, and compliance across the full lifecycle.
