Firmware is often the least visible part of a medical device - and one of the first places I would check for risk. If I had to boil this topic down, I’d focus on four things: knowing what’s inside the firmware, testing how it fails, checking how updates and boot security work, and tying every finding back to risk records and device history.
Here’s the short version:
- Visibility comes first. If I can’t identify firmware components, versions, and suppliers, I can’t map CVEs or sort fixes well.
- Basic testing is not enough. I need dynamic testing, fuzzing, and hardware checks to spot memory bugs, parser crashes, boot failures, and bad rollback behavior.
- Update security matters. Devices should verify signed firmware, block downgrades, protect keys in hardware, and avoid shared credentials.
- Traceability cuts delay. Every finding should link to hazards, requirements, tests, owners, and residual risk so teams can act without hunting through email and spreadsheets.
A few facts make the point fast:
- In lab testing cited in the article, about 50% of devices had unencrypted flash storage.
- Medical devices may stay in use for 10–20 years, far longer than most IT systems.
- New U.S. inspection pressure increased with FDA Compliance Program Manual #7382.850, effective February 2, 2026.
- The article also notes a major recall tied to firmware weaknesses that affected 465,000 pacemakers.
If I were building a firmware review process, I’d keep it simple:
- Inventory the firmware with binary analysis and SBOM review.
- Test failure paths with hardware-in-the-loop checks, fuzzing, and pen testing.
- Verify boot and update controls like signed updates, rollback protection, and hardware-backed key storage.
- Track each issue in one system with linked risk, test, and remediation records.
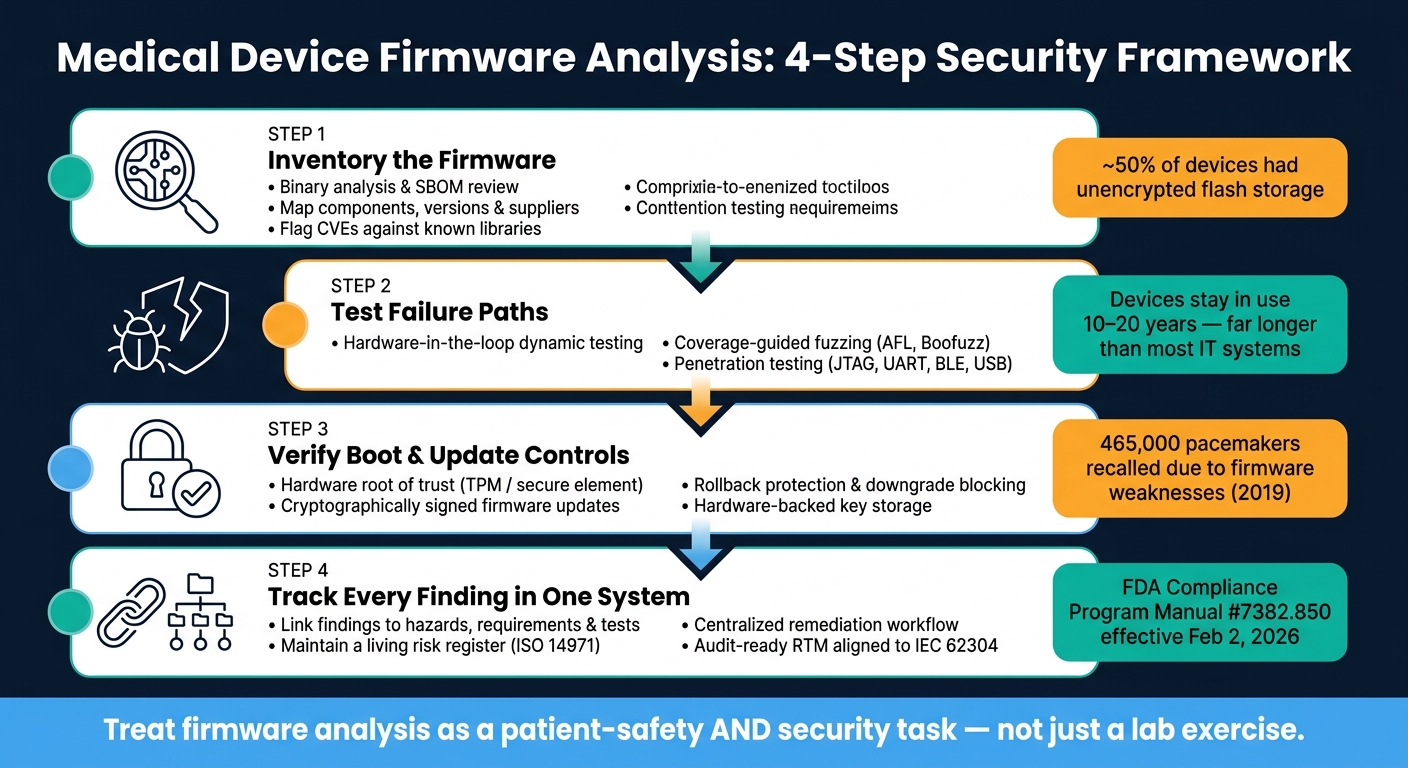
Medical Device Firmware Analysis: 4-Step Security Framework
Top 10 Medical Device Vulnerabilities with Myles Kellerman | Ep. 38
sbb-itb-535baee
Quick comparison
| Area | What I’d check | Main goal |
|---|---|---|
| Firmware visibility | Binary analysis, SBOMs, version mapping | Find components and known flaws |
| Security testing | Dynamic testing, fuzzing, pen testing | Find crash paths, logic bugs, and exploit chains |
| Device hardening | Secure boot, signed updates, key storage, least privilege | Stop tampering and unsafe installs |
| Governance | Risk management, RTM, and centralized tracking | Move fixes faster and support audits |
In short, I’d treat firmware analysis as a patient-safety and security task at the same time - not just a lab exercise.
Problem 1: Limited visibility into firmware contents and component origins
When source code isn't available, firmware analysis has to begin with compiled images and release metadata. That creates a blind spot fast. Compiled firmware images, patchy documentation, and old SBOMs can hide what the device is actually running. And if you can't tell where a component came from, it's hard to judge exposure or rank fixes the right way.
Solution: Combine static analysis, binary analysis, and software bill of materials review
The best approach is layered: use source analysis when code is available, binary analysis for compiled images, and SBOM review to map versions to known vulnerabilities.
Static source analysis checks embedded C and C++ for memory-safety flaws, logic mistakes, and insecure coding patterns. It's precise and can spot problems that disappear once code is compiled. The catch is simple: it needs full source access, and most healthcare teams don't have that for third-party or ODM firmware.
Binary analysis helps fill that gap. Tools like binwalk can unpack embedded filesystems such as squashfs, JFFS2, and ext2 from compiled images. String extraction can surface version markers and copyright notices. Hash and signature matching can compare binary chunks against databases of known libraries. Intel's cve-bin-tool, for example, can detect many embedded libraries, including OpenSSL and libpng [5]. A good first step is an entropy check with binwalk -E. High entropy often points to encryption, which may mean you need a hardware memory dump or decryption keys before you can go further [5].
SBOM review connects identified components to known vulnerabilities. For medical devices, CycloneDX fits firmware work well because it includes a native firmware component type and supports Vulnerability Exploitability eXchange (VEX) statements for postmarket monitoring [5][6].
"The regulators are flexible about tooling and format, but inflexible about completeness, accuracy, and the ability to act on the SBOM when a vulnerability is disclosed." - Nayan Dey, Senior Security Engineer, Safeguard [6]
Build a software bill of materials workflow for firmware releases
A firmware SBOM only helps if it stays current and links straight to device models and release versions. For in-house firmware, plug SBOM generation into the CI/CD pipeline with tools like Yocto's create-spdx or Buildroot. Every release should produce an inventory with git hashes, build timestamps, component hashes, and supplier and component identifiers such as PURL or CPE [7]. That inventory should also tie each component to a device model, release line, and vulnerability record.
For third-party or ODM firmware, binary-based generation is usually the main option. Tools like Syft can read internal package manager databases such as dpkg, apk, and opkg on embedded Linux devices. EMBA rolls extraction, binary hashing, and filesystem analysis into one audit workflow [5]. If a component can't be fully identified, mark it as unidentified instead of leaving a silent gap in the submission [6].
Procurement contracts should also require SBOM delivery from third-party suppliers. The final manufacturer is still responsible for the product's security posture, no matter who wrote the code [4][5].
Comparison table: Static source analysis vs. binary analysis vs. software bill of materials analysis
| Method | Primary Goal | Strengths | Limitations | Source Access Required | Best Use |
|---|---|---|---|---|---|
| Static Source Analysis | Find memory safety and logic defects | High precision; catches custom patches and logic errors | Requires full source code | Required | Internal R&D and pre-release audits |
| Binary Analysis | Identify components in compiled images | Works on third-party and legacy firmware | Lower confidence; may miss heavily modified code | Not Required | Auditing vendor firmware and field devices |
| SBOM Analysis | Inventory validation and CVE mapping | Scales well; ties components to vulnerability records | Only as accurate as the manifest or build metadata | N/A (uses manifest) | Procurement, postmarket monitoring, and fleet risk management |
Once the component inventory is clear, validate runtime behavior to catch defects binary review cannot prove.
Problem 2: Security defects missed by conventional testing
Once you know what components are in the device, the next step is to see how they break when something goes wrong. Functional testing tells you the device meets its spec. Dynamic testing shows what happens under malformed input, repeated failures, and interrupted updates. That difference matters.
Most standard test suites don't spend much time on those failure paths. And for medical devices that are network-connected, USB-enabled, wireless, or able to receive updates, that blind spot can turn into clinical risk.
Most device firmware is written in C or C++, which means memory-safety bugs can slip past routine testing and show up only when the device gets malformed input.
Solution: Apply risk-driven dynamic testing and hardware-in-the-loop validation
Start with the threat model and the ISO 14971 risk file. Then test the functions tied to patient safety, such as alarms, therapy output, authentication, and updates. That keeps the work focused instead of turning it into a giant test effort with no clear priority.
Use hardware-in-the-loop testing to check boot behavior, safe-state transitions, and rollback. Early checks can run in QEMU or FACT, but secure boot still needs to be confirmed on physical hardware. This ties boot integrity and rollback behavior directly to patient-safety outcomes. One practical validation step is to extract the firmware, change a non-critical component like a log string, re-flash it, and see whether the device refuses to boot [1].
Negative-path testing should be explicit and documented. A simple example: simulate 10,000 repeated authentication failures and check whether the audit log fills up or the device locks up. That's the kind of test that gives you traceability in a strict risk-management process. The FDA's Cybersecurity in Medical Devices Final Guidance, dated February 3, 2026, requires clear traceability between requirements, threat models, and testing results for premarket submissions [9].
That base makes fuzzing and penetration testing much more precise.
Add fuzzing and targeted penetration testing for firmware interfaces
Use coverage-guided fuzzing to hammer protocol parsers and interface handlers. Start with the interfaces most likely to take untrusted input:
- TCP/IP daemons
- Web interfaces
- USB
- BLE
- Device APIs
Frameworks like AFL and Boofuzz fit this job well.
Penetration testing takes things a step further by chaining weak points into realistic attacks on clinical devices. Look closely at JTAG, UART, authentication bypass, and privilege escalation paths. This kind of adversarial testing gives teams findings they can act on.
"Whether network connected or standalone, firmware is the center of controlling any embedded device. As such, it is crucial to understand how firmware can be manipulated to perform unauthorized functions." - OWASP Firmware Security Testing Methodology [8]
Comparison table: Dynamic testing vs. fuzzing vs. penetration testing
| Method | Defect Types Found | Lab Setup Needs | Required Skills | Lifecycle Phase | Evidence Produced |
|---|---|---|---|---|---|
| Dynamic Testing | Functional logic errors, safe-state failures, alarm malfunctions | Target hardware or high-fidelity emulator | Security/Clinical Engineering | Verification & Validation | Test logs, pass/fail requirements trace |
| Fuzzing | Memory corruption, parser crashes, buffer overflows | Protocol exercisers, fuzzing frameworks (AFL, Boofuzz) | Security Research / QA | Validation | Crash dumps, seed files, coverage reports |
| Penetration Testing | Authentication bypass, privilege escalation, RCE | Full system environment, network access | Independent Offensive Security Specialist | Validation / Pre-release | Pen-test report, findings ready for corrective action |
Use these findings to guide the next layer of firmware security review.
Problem 3: Weak firmware security controls and update mechanisms raise operational risk
Once testing shows where firmware can fail, the next step is simple: check whether the device can stand up to tampering and unsafe updates.
A lot of devices still fall short in familiar ways. There may be no secure boot. Credentials may be shared across devices or hard-coded into the system. Private keys may sit in flash without encryption. Some devices use a flat privilege model, which means every user gets admin-level power. And some update paths still accept unsigned firmware over cleartext channels.
That mix creates obvious risk. A bad actor may alter the device, knock it offline, or change behavior in ways that affect patient care.
A well-known case came in 2019, when the FDA recalled 465,000 St. Jude Medical (now Abbott) pacemakers because firmware weaknesses allowed unauthorized access. Attackers could have drained batteries or changed pacing settings. Patients had to go to a clinic to receive the firmware fix [3].
Solution: Verify secure boot, signed updates, key protection, and least privilege
Start with the boot process. The device should have a hardware root of trust, such as a secure element or TPM, that checks each boot stage with cryptographic validation. If that chain breaks, the device should not continue as if nothing happened.
Updates need the same level of care. Before installing any firmware, the device should verify a cryptographic signature.
"CRCs are not security controls. CRCs do not provide integrity or authentication protections in a security environment." - Nutfield Security [10]
Rollback protection matters just as much. Without it, an attacker can force the device back to an older firmware version that still has known flaws. Signing keys and TLS keys should live in hardware-backed storage, not in flash memory where they may be pulled out. Access rights should also match real job roles, so clinicians, service technicians, and administrators each get only the permissions they need.
Prepare healthcare teams for safe firmware update operations
Security controls on paper don't help much if update work falls apart in the field.
Use the SBOM to connect disclosed CVEs to deployed device models and firmware versions. From there, teams can sort issues by urgency: triage critical issues in 24–72 hours, high-severity issues in 30 days, and medium-severity issues in 90 days [3]. If patching has to wait because the device supports active care, use segmentation and monitoring as a stopgap until the update is in place.
Manufacturers can also cut down delays with a Predetermined Change Control Plan (PCCP). This lets pre-authorized security updates reach deployed devices without a full regulatory submission for every single patch [2].
Update behavior also needs to be predictable and auditable. If teams can't tell what changed, when it changed, or whether it worked, even a signed update process can turn into a mess.
Comparison table: Insecure vs. hardened firmware update practices
| Practice Area | Insecure Approach | Hardened Approach |
|---|---|---|
| Boot Integrity | No boot verification; accepts any flash image | Hardware root of trust; verifies each boot stage |
| Update Authentication | Unsigned updates or CRC checksums | Signed updates verified before install |
| Transport Protection | Updates over cleartext (HTTP/FTP) | Updates over encrypted channels (TLS 1.2/1.3) |
| Rollback Handling | No rollback protection; failed updates can brick the device | Auto-rollback to last known good version; downgrade attacks blocked |
| Credential Management | Hard-coded or shared admin passwords | Unique per-device credentials or certificate-based access |
| Clinical Workflow Impact | Unscheduled updates during patient care | Phased rollouts coordinated with planned maintenance windows [2] |
Problem 4: Poor traceability and fragmented risk governance slow remediation
Once firmware testing turns up a finding, traceability shapes how fast a team can act on it.
Even when testing spots a real firmware flaw, fixes often drag when ownership is split across security, clinical engineering, procurement, and compliance. Then the records end up scattered across different systems, inboxes, and spreadsheets. Findings sit in limbo. Ownership gets fuzzy. And medical device security risks can stay in service far longer than they should.
"If there is a single break in that chain [of traceability], the device may be considered non-compliant." - Ran Chen, Global MedTech Expert [11]
As of February 2, 2026, QMSR reinforces traceability from design inputs to outputs in U.S. federal requirements [11].
Solution: Link firmware findings to lifecycle evidence and risk records
This is where teams turn the firmware defects found in Problems 1–3 into action.
Each firmware finding needs a clear line from the issue itself to the records that matter. That means tying the finding to:
- the identified hazard
- the software safety requirement it violates
- the design module involved
- the verification test that shows the control works
- the residual risk assessment
A firmware finding only becomes actionable when it maps back to hazards, requirements, tests, owners, and residual risk.
Use an RTM aligned to IEC 62304 and ISO 14971, with each hazard, requirement, design module, and verification test explicitly linked.
A living risk register is what makes this work day to day. It should track each firmware issue by severity, IEC 62304 class, clinical impact, remediation status, compensating controls, and residual risk. Without that, change impact analysis turns into guesswork.
Use centralized risk management to coordinate medical device firmware oversight
Once the traceability chain is in place, route remediation through one workflow.
Censinet RiskOps™ can centralize vendor documentation, assessment findings, and remediation tasks in one place. That gives teams one shared view of what was found, who owns it, what still needs work, and what evidence supports closure.
Conclusion: Building a firmware analysis program for safer medical devices
A firmware analysis program depends on traceability, a living risk register, and centralized documentation.
When every finding is tied to a hazard, requirement, test, owner, and remediation status, teams can move faster, support audit readiness, and cut the risk of devices staying in service with unresolved firmware issues.
FAQs
How do I start firmware analysis without source code?
Start by getting a firmware dump from the device itself or by using firmware acquisition tools. Then convert that dump into a raw binary. From there, run a tool like binwalk to spot embedded files, file system markers, and other signatures, then extract what’s inside.
After that, open the binary in a hex editor and look for patterns, section boundaries, odd data blocks, and signs of weak spots. Automatic unpacking tools can help too, especially when the firmware is encrypted or uses a vendor-specific format. At every step, hands-on experience and knowledge of the device matter a lot.
Which firmware tests matter most for patient safety?
The most important firmware tests for patient safety focus on safety-critical functions like timing, accuracy, and alarm response. On top of that, system-level validation under real-world conditions helps check how the device behaves when it’s used the way people will actually use it.
The main priorities are regression testing, fault injection, and hardware-in-the-loop testing. Together, these tests help support reliable performance and effective risk control.
What records should each firmware finding link to?
Each firmware finding should link to records like:
- regulatory documentation required by FDA 52.304
- static analysis reports
- traceability matrices
- vulnerability management data, including SBOMs and verification evidence
That way, you have a clear paper trail for compliance and a more complete risk assessment.
