If you review healthcare AI like standard software, you can miss patient safety, PHI, and vendor-chain risk in one pass. My take is simple: before I approve any AI tool, I want a clear list of every model, API, dataset, cloud service, and subcontractor involved, plus proof of how the vendor tests, monitors, and limits PHI use.
Here’s the short version:
- Map the full AI stack: model owner, training data, speech or LLM APIs, cloud host, and subprocessors
- Match review depth to use case: radiology AI and sepsis scoring need more scrutiny than low-risk admin tools
- Lock down PHI terms early: BAAs should state training limits, retention rules, deletion timing, and subcontractor use
- Ask for AI-specific evidence: AI-BOM, model cards, subgroup testing, drift rules, rollback steps, and incident playbooks
- Check fourth parties: a vendor may look clean while passing data to other providers you never reviewed
- Keep monitoring after launch: model updates, drift, new subprocessors, and audit report changes should trigger review
A few facts make this urgent. In one well-known study, a health-risk algorithm gave fewer care resources to Black patients than White patients with similar needs because it used past cost as a proxy for health need. And in healthcare, a single hidden API can route PHI into systems your team never approved.
What I would not do is treat AI review as a one-time questionnaire. I would treat it as a lifecycle process: before contract, during rollout, and after go-live.
That means looking at six areas every time:
- Provenance - who built the model and what data shaped it
- Privacy - what PHI enters the tool, where it goes, and how long it stays
- Safety - how the vendor tests outputs, errors, and subgroup performance
- Security - prompt injection, data poisoning, model theft, and access controls
- Dependencies - cloud hosts, upstream model APIs, and data brokers
- Monitoring - drift alerts, version change notices, and annual rechecks
| Area | What I look for first | Red flag |
|---|---|---|
| Model source | AI-BOM and model card | Vendor cannot name upstream models |
| PHI use | BAA limits on training and retention | Vague training or deletion terms |
| Clinical testing | Subgroup results and validation studies | No population-specific evidence |
| Security | MFA, encryption, runtime patching, attack testing | No AI-specific threat review |
| Fourth parties | Subprocessor list and API disclosure | Hidden speech, LLM, or cloud vendors |
| Post-launch checks | Drift thresholds and rollback plan | No update notice or revalidation plan |
Bottom line: if a vendor cannot show where the model came from, where the data goes, how outputs are tested, and who else is in the chain, I would slow the deal down or stop it.
Below, I break that into a simple review framework teams can use in procurement, legal, privacy, security, and clinical governance.
Security for the AI supply chain ft. Aeva Black | Technically Speaking with Chris Wright
The New Baseline: Regulatory, Privacy, and Governance Expectations
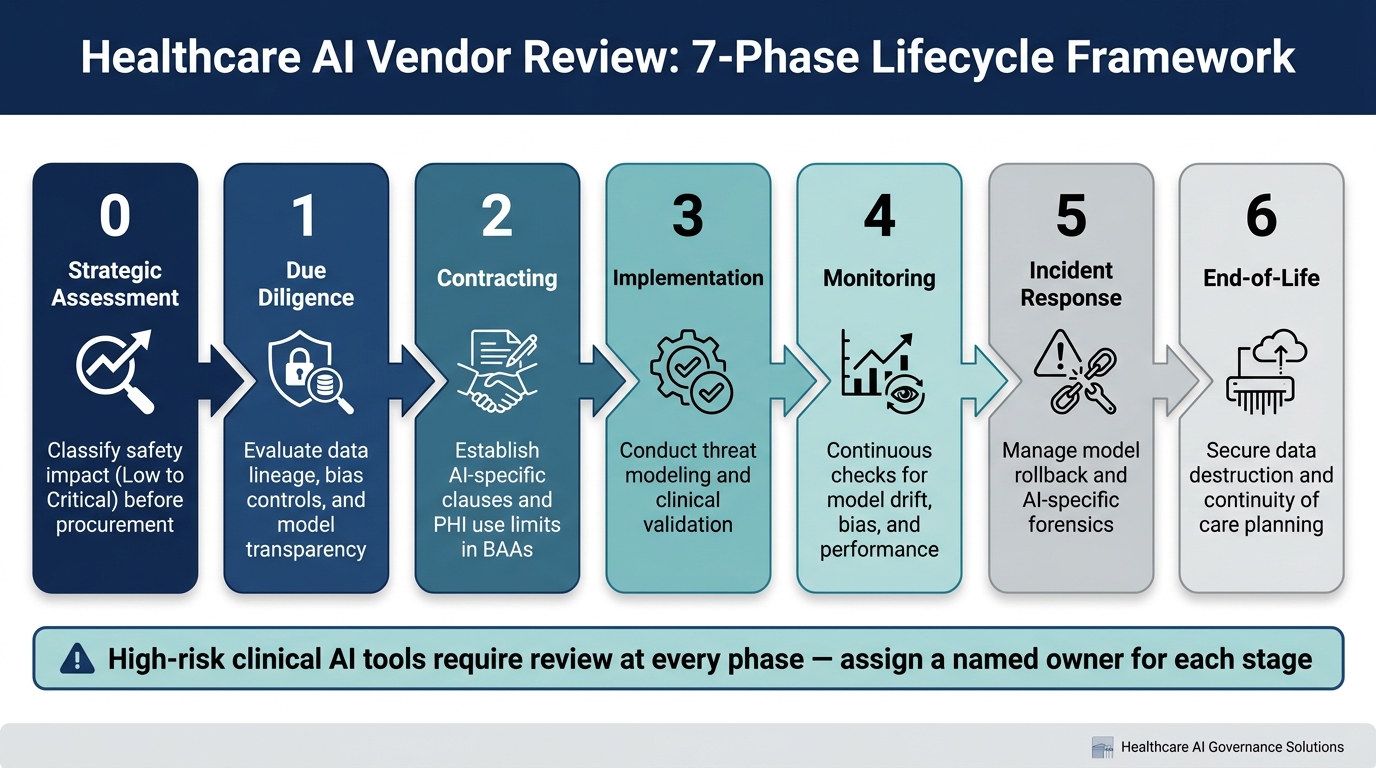
Healthcare AI Vendor Review: 7-Phase Lifecycle Framework
The bar for reviewing AI vendors has changed. After you map the supply chain, the next step is regulatory and governance controls. A vendor might clear a standard security review and still leave major AI risk out of sight. That’s why AI vendor review can’t be treated like a one-and-done checklist. It has to work across the full vendor lifecycle.
This changes the job, too. Review is no longer just a static compliance exercise. It becomes continuous governance.
Traditional vendor reviews miss AI systems that learn, drift, and rely on opaque supply chains. [2]
BAAs and PHI Use Limits in AI Workflows
Start with the contract. In healthcare AI, PHI limits shape every control that comes after. The BAA should spell out how PHI can be used, whether the vendor can use it to train models, and how long that data can stay in the system.
When reviewing a BAA for an AI supplier, focus on a few core points:
- PHI use boundaries: training, fine-tuning, reuse, and subcontractors
- Retention and deletion: timelines for removing PHI from inference logs, training pipelines, and support systems
- Vendor and provider obligations: performance, monitoring, and incident response
If those terms are fuzzy, the rest of the review gets shaky fast.
Use a Lifecycle Review Model
A seven-phase lifecycle gives teams a clear way to handle procurement, rollout, and monitoring without treating them as separate jobs. It also makes ownership easier to assign and follow-up easier to trigger.
| Phase | Focus Area | Key Action |
|---|---|---|
| Phase 0 | Strategic Assessment | Classify safety impact (Low to Critical) before procurement |
| Phase 1 | Due Diligence | Evaluate data lineage, bias controls, and model transparency |
| Phase 2 | Contracting | Establish AI-specific clauses and PHI use limits in BAAs |
| Phase 3 | Implementation | Conduct threat modeling and clinical validation |
| Phase 4 | Monitoring | Continuous checks for model drift, bias, and performance |
| Phase 5 | Incident Response | Manage model rollback and AI-specific forensics |
| Phase 6 | End-of-Life | Secure data destruction and continuity of care planning |
Use this lifecycle to assign ownership and set follow-up points. Before procurement, classify each AI use case by safety impact. A low-risk admin tool does not need the same depth of review as clinical decision support. Still, every use case needs a named owner, clear review rules, and monitoring in place.
Core Criteria for Assessing AI Supply Chain Integrity
AI supply chain reviews need to go past static software checks. Models drift. They rely on upstream services. And they can introduce risks that a standard vendor questionnaire simply won't catch. Use the criteria below to decide whether a vendor should be approved, approved with limits, or rejected. For high-risk clinical use, missing provenance, subgroup validation, or fourth-party disclosure should stop approval.
| Review Dimension | Legacy Criteria | AI-Specific Criteria |
|---|---|---|
| Software inventory | Static SBOM, version control | AI-BOM, embedded APIs, foundation model dependencies |
| Testing and validation | Functional QA, user acceptance testing | Subgroup performance testing, bias checks, real-world clinical validation |
| Data controls | Data classification, access controls | Training data lineage, consent documentation, PHI segregation, labeling audit trails |
| Change management | Patch management, release notes | Retraining triggers, rollback options, governance approval for model updates |
| Security assessment | Network controls, encryption, incident response | Prompt injection defenses, data poisoning resilience, model theft protections, unsafe plugin integrations |
| Third-party visibility | Primary vendor security attestation | Fourth-party disclosure: cloud hosts, upstream model APIs, data brokers |
| Ongoing monitoring | Uptime SLAs, vulnerability scans | Drift detection thresholds, adverse event reporting, periodic revalidation |
Model Provenance, Data Lineage, and Technical Transparency
Start with provenance. If you don't know what the model is built from, the rest of the review is standing on shaky ground.
The first question for any AI vendor should be simple: who built this model, and with what data? That answer is often spread across several vendors. In healthcare, buyers need enough traceability and auditability to see whether the system is a fine-tuned foundation model, which external APIs it calls, and which datasets were used for pretraining and fine-tuning.
Ask vendors for an AI Bill of Materials (AI-BOM) that lists every model owner, training data source, embedded API, and cloud dependency, along with version history and change-control processes. If that documentation is missing, treat it as a serious gap, not a small paperwork issue. Pair it with a model card that spells out intended use, known failure modes, performance by demographic subgroup, and monitoring plans. If there's no model card, that should block clinical procurement. Otherwise, you're buying a system without a clear view of its training data, limits, or failure modes.
Data lineage matters just as much. You need direct answers to a few basic questions:
- Where did the training data come from?
- How was it collected, labeled, and de-identified?
- What usage rights apply to that data?
- Was PHI kept out of training pipelines?
Those answers shape HIPAA exposure and determine whether the system can be audited in a serious way.
Bias, Clinical Safety, and Post-Deployment Monitoring
Pre-deployment testing matters, but it isn't enough. A model can look solid in a vendor's test setting and still perform very differently with your patient population.
That risk isn't abstract. Research on a widely used health management algorithm found that it allocated fewer resources to Black patients than White patients with similar health needs because it used past healthcare costs as a proxy for health status, embedding structural inequity into its predictions. [3]
Before deployment, require subgroup performance metrics. After deployment, require drift thresholds, adverse-event reporting, and annual revalidation.
Safety review also has to look at the attack surface. That's where many teams get caught off guard.
Cybersecurity, Infrastructure, and Fourth-Party Dependencies
AI systems open up attack paths that standard security reviews often miss. Prompt injection, where malicious input changes model behavior, is a real risk for any AI tool tied to EHR workflows. Data poisoning can corrupt model training with adversarial samples, even at small scale. Add model theft and unsafe plugin integrations, and the threat picture starts to look very different from a standard SaaS app.
On the infrastructure side, require environment separation, MFA, and role-based access for all human and system accounts that can access PHI. Require encryption in transit and at rest. And make sure patching covers AI runtime libraries, not just application code. That's an easy detail to miss.
For fourth-party dependencies, ask for full disclosure of cloud hosts, upstream model API providers, and data brokers, along with their security attestations and incident response commitments. If an AI vendor depends on a major cloud LLM API, your team needs to review that API's data retention policies, geographic data residency, and incident history before any PHI moves through it.
Turn these criteria into questionnaire items, scorecard fields, and contract terms in the next section.
sbb-itb-535baee
How to Run the Review: Questionnaires, Checklists, Scorecards, and Contracts
The goal here is simple: turn AI review into a process your team can run the same way every time.
That means using the same risk areas from your earlier review - provenance, PHI handling, third-party dependencies, safety testing, monitoring, and incident response - and turning them into three working tools:
- an intake questionnaire
- a scoring method
- a contract review checklist
When those three pieces line up, vendor review gets a lot less messy. You’re not judging each tool from scratch. You’re checking whether the supplier can show clear proof in the areas that matter most.
AI-Specific Vendor Questionnaires and Evidence Requests
Build the questionnaire around the same risks that drive AI review: provenance, PHI handling, third-party dependencies, safety testing, monitoring, and incident response. Use a dedicated AI questionnaire that maps each risk domain to evidence.
| Questionnaire Domain | Key Questions | Evidence to Request |
|---|---|---|
| PHI handling | Which PHI does the tool access? Is PHI used for training? | Data protection addendum, retention schedules, de-identification documentation |
| Model origin and provenance | Is the model in-house, licensed, or built on a foundation model? What training data sources are used? | Model cards, documentation of model lineage, validation studies by use case and subpopulation, software bills of materials (SBOMs) for AI components |
| Data controls | How is minimum necessary access enforced? What encryption is used? | SOC 2 Type II report and related control documentation |
| Third- and fourth-party dependencies | Which cloud platforms or model APIs does the solution rely on? | Subprocessor list, SOC 2 or ISO 27001 reports for key dependencies |
| Security architecture | What protections exist against prompt injection and data poisoning? | Network architecture diagrams, penetration test summaries |
| Safety testing and clinical validation | Which performance and bias metrics are tracked? How is bias evaluated? | Validation studies, bias and robustness assessments |
| Monitoring and lifecycle management | How is drift detected? How are customers notified of model updates? | Telemetry dashboard examples, model versioning and rollback procedures |
| Incident response | Which events trigger safety or security notification? What are notification timelines? | Sample incident response playbooks for cyber, privacy, and safety events |
Missing or vague responses in any of these areas should count as a risk finding. If a vendor can’t produce a model card or a subprocessor list, that’s not a paperwork issue. It’s a transparency gap that affects the rest of the review.
Governance Scorecards for Procurement and Risk Acceptance
Score each supplier on privacy, security, safety, transparency, resilience, and residual risk using a weighted 1–5 scale. For clinical use, any score below 3 on safety or privacy should trigger AI governance committee review. Scores above a defined risk threshold should limit deployment to a pilot phase or require compensating controls before broader rollout. Route high-risk findings to the AI governance committee and track remediation in a single workflow.
In practice, the scorecard should do more than label a vendor as “good” or “bad.” It should drive the next step. A weak privacy or safety score means the deal needs more review. A high residual risk score may mean the tool can only be used in a controlled pilot. And if the gaps can be managed, the scorecard should show which compensating controls are needed before launch.
Use the scorecard outcome to decide which clauses must be mandatory before approval.
Contract Clauses That Matter for AI Suppliers
Contract review is where governance expectations become legally enforceable. Address PHI use limits, data ownership, fourth-party disclosure, model-update notice, audit rights, incident timelines, data destruction, and AI-specific indemnification.
Indemnification language needs close review. If an AI vendor's model produces a harmful output that contributes to a patient safety event, the contract should define liability clearly - including whether the vendor's indemnification covers AI-specific failures, not just standard software defects. This is where the paper review becomes something your organization can enforce. Without these terms, even a well-documented vendor review doesn’t give you much protection when something goes wrong.
The table below maps each review stage to required evidence and accountable owners.
| Review Stage | Required Evidence | Accountable Stakeholders |
|---|---|---|
| Pre-contract | AI-specific questionnaire responses, model cards, SBOMs for AI components, SOC 2 reports, pen test summaries, validation studies, subprocessor lists | Procurement, security, privacy, clinical |
| Contracting and approval | Executed BAA, AI use restriction clauses, data ownership terms, subcontractor disclosure, model update governance, audit rights, incident reporting windows | Legal, privacy, security |
| Post-deployment monitoring and renewal | Drift detection reports, incident logs, model update notifications, annual revalidation studies, updated SOC reports | Security ops, clinical informatics, compliance |
Building a Repeatable AI Supply Chain Risk Program
Once a vendor gets approved, the work doesn't stop. It shifts into a steady operating rhythm.
Vendor review is not a one-and-done step. Treat AI supply chain review as an ongoing program, because models change, dependencies shift, and requirements don't sit still.
Don't spin up a separate AI process if you can avoid it. Instead, build AI-specific checks into the workflows your team already uses: third-party risk assessments, security reviews, privacy impact assessments, procurement approvals, and clinical governance. When AI provenance questions sit inside your standard vendor questionnaire, and PHI handling checks show up in every BAA review, the process is much easier to run at scale.
Clear ownership matters here. The CISO should own security and incident response. Privacy and compliance should handle HIPAA and BAA review. Clinical leadership should manage safety sign-off. Procurement should handle supplier follow-up. Set escalation paths before procurement begins. Those owners should also get monitoring reports, incident notices, and remediation updates on a fixed schedule.
Continuous Monitoring and Governance Ownership
After launch, shift from upfront evaluation to scheduled monitoring. Track model version changes, dependency changes, including new subprocessors or cloud migrations, updated audit reports, and performance drift on a set schedule. High-risk clinical AI tools should get reviewed quarterly. Lower-risk, non-clinical tools can follow an annual cycle, with ad hoc reviews triggered by material changes or incidents. HSCC guidance calls for preplanned incident response, reporting channels, and continuous monitoring.[1]
You should also track subgroup performance by age, gender, race, ethnicity, and socioeconomic status. The goal is simple: watch for unequal outcomes as part of your post-deployment routine, not just during a one-time validation check. Assign a named owner, pick a review frequency, and spell out what triggers escalation.
A centralized workflow helps keep this from turning into a mess. Use it to track evidence, integrations, and fourth-party exposure across vendors. Then feed new evidence, incidents, and regulatory changes back into the next review cycle.
FAQs
What makes AI vendor review different from standard software review?
AI vendor review is different from a standard software review because AI isn’t a fixed product. It changes over time. And that means the risk changes too.
With regular software, you’re often checking a system that works the same way day after day. AI is different. Performance can shift. Outputs can drift. New issues can show up after launch, including model drift, data leakage, and bias. That’s why review can’t be a one-time box to check. It needs steady oversight.
Reviews also have to look at more than the tool itself. They need to examine the full AI supply chain, including model provenance, training data controls, and post-deployment monitoring. If you skip those pieces, you’re only seeing part of the picture.
A solid review process should also include risk-based governance, contract terms that cover audit rights and model changes, and input from the teams that will deal with the fallout if something goes wrong, such as clinical, legal, and security.
When should a healthcare AI vendor be rejected or limited to a pilot?
Reject a healthcare AI vendor outright, or keep them limited to a pilot, if they can’t provide basic AI supply chain proof. That includes model lineage, training data provenance, and clear disclosure of subcontractors and fourth-party dependencies.
Approval should also stop if the vendor has no documented testing for data poisoning, model evasion, or data leakage. The same goes if they refuse to sign a required Business Associate Agreement (BAA) for any workflow that involves Protected Health Information (PHI).
How often should healthcare organizations re-evaluate AI vendors after launch?
Re-evaluation frequency should match the tool’s risk profile. High-risk AI vendors should be reviewed quarterly. Lower-risk vendors can be reviewed annually.
That schedule works best when it’s backed by continuous monitoring. In practice, that means tracking model drift, performance metrics, and security incidents as they happen, not just during a formal review window.
It also helps to review the full vendor portfolio once a year. Regulations change, and fast-moving AI tools can shift from low concern to higher concern before you know it.
