AI can fail while the EHR still looks fine - and that can put patients, staff, and revenue at risk. I’d boil this article down to one point: if a hospital uses AI in care, it needs a clear plan for when that AI is wrong, slow, missing, or compromised.
Here’s the short version:
- AI incidents are climbing. Reported AI safety incidents went from 149 in 2023 to 233 in 2024, a 56.4% jump.
- A normal EHR downtime plan is not enough. AI tools can break on their own, even when the main record system is still online.
- The biggest risks are easy to miss. Think missed sepsis alerts, made-up note content, drift in model output, cyber events, and vendor outages.
- The damage spreads fast. One bad AI output can affect charts, orders, coding, quality reporting, throughput, and billing.
- Most of the gap is about ownership. If no one clearly owns detection, shutdown, fallback, and restart, response slows down when time matters most.
- What needs to be in place now: incident playbooks, manual fallback steps for high-risk workflows, tighter vendor terms, and routine review after go-live.
If I were leading a health system, I’d want clear answers to four questions right now:
- How do we know an AI tool is failing?
- Who can stop it?
- What manual workflow starts right away?
- What must happen before it goes back into use?
That’s the heart of the piece: AI failure is not just an IT problem. It is a patient safety, care continuity, and financial risk issue that needs named owners and written response steps.
The AI Failure Scenarios Health Systems Have Not Planned For
The failure modes that matter most are operational, clinical, and easy to miss. They interrupt care, warp records, and slow response without setting off a loud alarm. In many cases, there’s no obvious outage at all. The first signs show up in day-to-day clinical work.
Missed Alerts, Hallucinated Documentation, and Silent Model Drift
When a sepsis alert doesn’t fire, or fires too late, the damage goes far beyond a missed message. It can mean delayed antibiotics, longer ICU stays, and a patient safety event that never gets tied back to the model. The same pattern shows up with other high-risk alerts, including sepsis, stroke, respiratory decline, and post-op deterioration. If alerts fail quietly, clinicians lose the safety net they thought was there.
Hallucinated documentation creates a different kind of danger. A generative AI tool can produce a note that invents a medication history, makes up an allergy, or gets the visit details wrong. On the surface, the note may look fine. That’s the trap. A plausible note can move through the chart unchecked and then shape medication orders, quality reporting, and medico-legal records [2][1]. The risk grows when no one is checking whether the model’s output is still accurate over time.
Silent model drift is one of the hardest problems to spot. A Stanford summary of hospital AI documentation found that models were poorly documented for reliability, fairness, and performance over time, covering barely 40% of 220 individual recommendations across 15 reporting guidelines [1]. In one University of Michigan model tested on 30,000 patients, the system missed about two-thirds of actual cases while also producing many false alarms [1]. The system didn’t crash. It just stopped doing the job well. That turns monitoring into a resilience problem, not only a model-quality problem.
Cyber Incidents and Vendor Outages That Break AI-Dependent Care Processes
Ransomware now hits more than EHR access. It also breaks AI-dependent workflows. A Proofpoint survey cited by Zentera found that 70% of healthcare organizations hit by ransomware reported patient care disruption [4]. When ambient documentation tools, radiology prioritization queues, or prior authorization engines go down, clinical teams often don’t have a practiced manual backup. They make it up as they go, and that leads to documentation backlogs, slower throughput, and revenue cycle delays.
API failures and SaaS outages cause much the same kind of damage, even without the drama of a ransomware attack. A radiology workflow disruption reported by Radiology Business showed that a cyber outage forced radiologists to transcribe reports by hand and delay nonurgent cases, slowing throughput and report turnaround [3]. This isn’t some edge case. It’s what happens when clinical workflows depend on third-party AI services and no one plans for downtime. Without clear fallback ownership, the outage stops being just an IT issue and becomes a care-process failure.
How AI Failures Spread Beyond the Original Tool
AI failures are so disruptive because the output rarely stays inside the tool that made it. Errors can move into charts, coding, utilization review, quality reporting, bed management, and billing. Once that happens, the original problem starts to branch out. A bad output in one place can shape decisions somewhere else.
Health systems that haven’t mapped those downstream dependencies may not yet see how far the impact goes for tools already in use. And when ownership isn’t clear, those downstream effects spread faster than the first failure.
The next issue isn’t only the failure itself. It’s who has to detect it, escalate it, and stop it. These cascades get worse fast when no one owns the response, escalation, or rollback.
sbb-itb-535baee
The Gaps in Ownership, Oversight, and Vendor Risk That Make AI Failures Worse
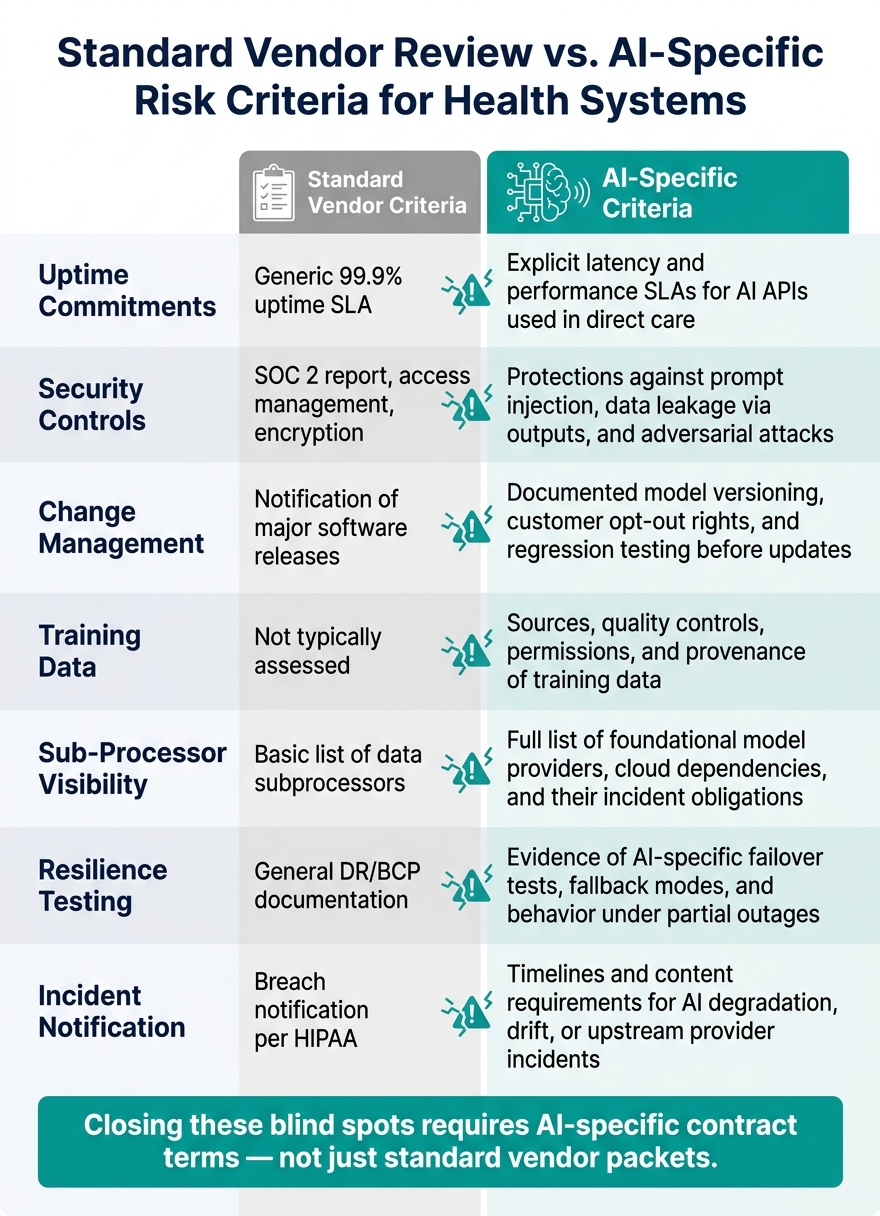
Standard Vendor Review vs. AI-Specific Risk Criteria for Health Systems
AI failures turn into high-impact events when no one clearly owns detection, containment, and recovery. In many health systems, clinical, IT, and vendor teams all do part of the work, but no single group carries the accountability.[5] When that happens, the first warning sign usually isn't the failure itself. It's the slow response.
No AI Downtime Procedures, No Clear Escalation Paths, No Monitoring
Generic IT downtime plans don't cover partial AI degradation, version drift, or output-level hallucinations. So a risky failure can keep going without setting off any response.
Picture the moment a clinician notices odd AI behavior. Who do they call first - the help desk, the vendor, or clinical informatics? In many cases, there isn't a clear answer. The issue turns into a ticket, sits in limbo, or disappears altogether.
Teams need to track more than whether the system is "up." They should log:
- Latency
- Hallucination or error rates against a validated sample
- Override rates
- Version changes
- Input characteristics
- Timestamps
- Downstream actions
Those records make it possible to reconstruct an incident, identify the failed version, and trace what happened after the bad output. That's why monitoring and escalation are the first resilience controls to put in place.
Weak Clinician Guardrails and Governance Checkpoints
In 2024, 74% of U.S. hospitals reported shared accountability for predictive AI, but only 66% had a dedicated committee or task force.[7] Shared accountability with no clear owner is, in practice, close to no ownership at all.
A lot of health systems still let vendors push model updates with little formal review. No pre-deployment safety check. No multidisciplinary sign-off. No regression testing against known clinical scenarios. That's a risky way to run high-stakes tools.
For high-risk use cases like sepsis alerting, imaging interpretation, and medication dosing support, governance committees led by CIOs, CMIOs, CISOs, and compliance leaders should handle major AI changes the same way they handle new medication formulary additions or new device introductions. That means documented risk assessments, explicit sign-offs, and approval decisions before anything reaches patients.
Those checkpoints are what keep unsafe AI changes from slipping into care.
AI Vendor and Fourth-Party Risk Blind Spots
Standard vendor reviews in U.S. health systems usually focus on HIPAA compliance, basic security controls, and general uptime SLAs. That's fine for ordinary software. It's not enough for AI.
The Health Sector Coordinating Council has warned that AI-driven supply chains are outpacing healthcare cybersecurity defenses because AI systems bring model drift, training data dependencies, algorithmic bias, and multi-vendor supply chains that old software reviews don't address.[6]
The dependency chain is also bigger than it looks. About 80% of hospitals using predictive AI rely on models from their EHR vendor, and roughly 52% use added models from other vendors.[8] So even if a health system only has a contract with the immediate vendor, upstream model changes, throttled API access, or cloud outages can still degrade AI performance inside the organization.
The table below shows the gap between standard vendor reviews and what AI deployments need:
| Assessment Area | Standard Vendor Criteria | AI-Specific Criteria |
|---|---|---|
| Uptime commitments | Generic 99.9% uptime SLA | Explicit latency and performance SLAs for AI APIs used in direct care |
| Security controls | SOC 2 report, access management, encryption | Protections against prompt injection, data leakage via outputs, and adversarial attacks |
| Change management | Notification of major software releases | Documented model versioning, customer opt-out rights, and regression testing before updates |
| Training data | Not typically assessed | Sources, quality controls, permissions, and provenance of training data |
| Sub-processor visibility | Basic list of data subprocessors | Full list of foundational model providers, cloud dependencies, and their incident obligations |
| Resilience testing | General DR/BCP documentation | Evidence of AI-specific failover tests, fallback modes, and behavior under partial outages |
| Incident notification | Breach notification per HIPAA | Timelines and content requirements for AI degradation, drift, or upstream provider incidents |
Closing these blind spots means negotiating AI-specific contract terms, not just relying on a standard vendor packet. Health systems need prompt incident notification, sub-processor disclosure, joint post-incident reviews, and the right to pause or roll back model updates when internal validation shows safety concerns.
Without those terms, the hidden vendor risk doesn't disappear. It just gets pushed onto the health system. These are the blind spots that shape the triggers, fallback rules, and review criteria health systems need next.
What to Build Now: AI Failure Playbooks, Fallback Workflows, and Risk Criteria
These failures become manageable only when health systems turn them into named response playbooks, fallback workflows, and review criteria. The goal isn't broad policy language. It's three concrete controls: incident playbooks, fallback workflows, and lifecycle risk criteria.
AI Incident Response Playbooks with Clear Triggers and Severity Levels
An AI incident response playbook is a cross-functional runbook shared by clinical, operational, legal, and security teams. It should name who owns what and set time targets for escalation.
The playbook needs to spell out triggers, severity tiers, escalation paths, containment steps, recovery checks, and documentation. Severity should be based on patient harm, scope, time to detection, and reversibility. A hallucinated note caught before any treatment decision is lower severity than a misclassified radiology triage output that delays care across a service line.
Tie the playbook to the failure modes already showing up: missed alerts, hallucinated notes, model drift, and vendor outages. It should answer a few plain questions: Who can disable the tool? Who alerts clinical leadership? What has to happen before the tool is safe to turn back on? Re-enable only after the root cause is confirmed, output matches a known-safe baseline, and both clinical and technical owners sign off.
When an AI tool fails, the response must shift at once from alerting to manual care.
Fallback and Rollback Workflows for High-Risk Care Processes
The top fallback workflows should cover the care processes already on the table: ED triage, clinical documentation, imaging prioritization, sepsis alerting, and medication verification. Each one needs a defined manual fallback, a rollback trigger, and a reactivation checkpoint before AI use starts again.
| AI Failure Type | Clinical Impact | Required Playbook Components |
|---|---|---|
| Triage model unavailable | Delayed acuity classification; missed high-acuity patients | Revert to standard triage protocol and manual intake workflow |
| Documentation model hallucination | Wrong treatment decisions if chart is trusted | Switch to templated human-authored notes; flag affected encounters for review |
| Imaging prioritization failure | Delayed reads for time-sensitive studies | Revert to acuity-based routing or direct radiologist review |
| Sepsis alert model drift | Delayed sepsis recognition or over-treatment | Suspend model; revert to manual screening criteria |
| Medication verification AI outage | Greater risk of error during verification | Activate manual verification workflow and recheck each step |
Fallback procedures help, but they aren't enough on their own. Leaders also need criteria before and after deployment that catch drift before it reaches patients.
Minimum AI Risk Assessment Criteria Before and After Deployment
Before go-live, leaders should ask for evidence of clinical safety testing across relevant patient subgroups, defined drift monitoring thresholds, audit logging, human oversight requirements, documented downtime procedures, vendor notification obligations, and traceability back to source data. They should also confirm that failure modes have been analyzed and that staff know what to do when the AI is wrong or unavailable.
AI review should be treated as a lifecycle control, not a one-time check. Teams should review override rates, drift, and clinician concerns on a regular basis, then review again after any EHR update, model change, or workflow shift. For sepsis models, monitor AUROC, precision, recall, false-positive rate, and drift continuously, with real-time alerts that trigger governance action when performance degrades [9]. That is the control that keeps earlier failures - missed alerts, hallucinated documentation, and model drift - from moving into patient care, records, coding, and operations.
These controls work only when one team owns intake, review, and monitoring across the AI lifecycle.
Building a Continuous AI Resilience Program with Censinet
These controls matter only if someone still owns them after go-live. managing third-party AI risk has to stay tied to vendor oversight, governance, and enterprise risk. That means treating missed alerts, hallucinated documentation, model drift, ransomware outages, and vendor disruption as day-to-day operating risks, not a box checked during approval. The next move is simple: turn those controls into a living operating model.
Use Censinet RiskOps to Centralize AI Risk Oversight and Vendor Assessments
Censinet RiskOps™ can act as the central system of record for AI risk oversight. It keeps a central AI inventory with owners, use case, data type, workflow, and deployment status. So if a team runs into missed alerts, hallucinated notes, or model drift, those issues can be tied back to the right owner and workflow fast. It also tracks vendor assessments, remediation tasks, and resilience documentation.
As AI-enabled devices and tools keep piling up, health systems need a way to track what each one actually does. RiskOps can map each tool to triage, documentation, sepsis alerting, scheduling, and revenue cycle. That way, vendor changes and upstream outages are already linked to downstream impact.
With that inventory in place, teams can move reviews faster without giving up oversight.
Use Censinet AI and Censinet AITM to Speed Review While Keeping Humans in Control

Censinet AITM™ helps move questionnaires, evidence summaries, integration details, and upstream dependency risk reviews along faster. The 2026 HSCC guide requires vendors to report security incidents, degradations, and model anomalies within the incident-response timeline. [12]
Censinet AI helps send AI-related findings to the right people. PHI issues can go to privacy and compliance. Security issues can go to the CISO team. Workflow issues can go to CMIO and nursing leadership automatically. [10][6][11] Risk teams set the routing rules, but people still make the final calls. That means each finding reaches the right reviewer and goes through a documented approval before any action happens. The result is a review process that keeps moving while escalation stays clear.
Conclusion: Health Systems That Plan for AI Failure Will Be the Safest
AI failure is not some abstract IT problem. It is a patient safety issue, a compliance exposure, and a care continuity risk. And many health systems still have not built the controls needed to manage it. The path forward starts with identifying hidden failure modes, assigning named owners, setting incident triggers, building fallback workflows, tightening vendor criteria, and making oversight continuous instead of one-time approval. Health systems that treat AI resilience as an operating discipline - not a checkbox - will be in a stronger position to protect patients, limit legal exposure, and keep care running when AI tools fall short.
FAQs
How is AI downtime different from EHR downtime?
AI downtime is different because the system can look fine while still giving unsafe advice, biased suggestions, or flawed documentation.
That’s what makes it tricky.
With an EHR outage, the problem is usually obvious. The system crashes, alerts fire, and teams know something is wrong right away. AI failures don’t always show up like that. They can stay quiet in the background through model drift, weaker output quality, or bias.
And because those issues are harder to spot, they often take more time to catch. Fixing them also isn’t just an IT job. It usually takes a cross-functional response, with input from technical teams, clinical staff, compliance, and other stakeholders that a standard outage may not involve.
Which AI failures pose the highest patient safety risk?
Failures in AI that guide clinical decisions, especially in triage and diagnostic support, carry the highest patient safety risk.
Here’s the core issue: if an AI system labels a critically ill patient as low acuity, or misses a subtle condition that a clinician needed to catch, care can slow down at exactly the wrong moment. That delay can lead to the wrong treatment, serious harm, or death.
The risk gets even worse when AI offers treatment advice, such as dosage recommendations, that is wrong because the system was trained on poor data. If clinicians lean on those outputs without checking them closely, bad guidance can turn into bad care fast.
What should a hospital include in an AI fallback plan?
A hospital’s AI fallback plan should clearly map each clinical service to the systems, vendors, and data it relies on. It should also spell out who has the authority to pause, override, or shut down high-risk AI when performance slips or safety thresholds are crossed.
That plan needs to cover manual workflows, escalation paths, technical recovery controls, vendor contingency procedures, and clinician override mechanisms that have been validated in practice. It should also include regular drills so teams can test downtime transitions and make sure restoration happens safely.
