If you work in healthcare, the main point is simple: use blockchain to verify identity, not to store PHI. Keep patient data off-chain, use DIDs and verifiable credentials to prove claims, and add selective disclosure so people share only the data needed for each step.
Here’s the short version:
- Centralized identity creates one big target for breaches and account misuse.
- Blockchain works better as a trust layer for keys, credential status, and issuer checks.
- Patients, clinicians, staff, devices, and vendors all need identity controls.
- PHI should stay off-chain in EHRs, HIEs, wallets, or secure cloud systems.
- Pairwise DIDs, revocation registries, and zero trust checks help limit tracking and misuse.
- OAuth 2.0, OpenID Connect, SMART on FHIR, and EHR APIs still have a place; this model extends current IAM instead of replacing it.
- Early use cases include consent, provider directories, audit logs, prior auth, and vendor access.
- Rollout works best in phases: assess gaps, run a tight pilot, then scale with governance and risk review.
A few facts stand out. Only 5.7% of organizations report full visibility into service accounts. 79% have had secrets leaks, and 77% of those incidents caused damage. On the compliance side, Information Blocking penalties can reach $1,000,000 per violation. That makes identity, audit trails, and revocation more than just IT tasks.
If I had to boil the article down to one line, it would be this: put trust data on-chain, keep health data off-chain, and build clear rules for issuance, use, and revocation from day one.
Blockchain Identity Rollout Roadmap for Healthcare Organizations
Decentralized Identity (DID): The Blockchain Revolution in Healthcare
sbb-itb-535baee
1. Core Concepts HDO Leaders Need to Know
HDO identity management has to verify patients, clinicians, staff, and devices across many systems. In a blockchain-based model, the chain stores identity metadata, public keys, credential schemas, and revocation status. PHI stays off-chain. That setup creates a trust layer for both people and connected systems.
Compared with centralized IAM, blockchain-based identity changes where trust sits. Instead of leaning on one central system, it leans on cryptography, portable credentials, and off-chain PHI storage.
Digital identity for patients, clinicians, staff, and devices
Every HDO access point runs on identity: patient portals, EHRs, telehealth, and connected devices. For patients, identity is built around DIDs tied to verified demographics and, when needed, medical power of attorney. For clinicians, identity depends on licenses, diplomas, and specialty credentials checked by the issuing authority. Staff identity controls access to admin systems and vendor connections.
Devices need identities too. They log into the same environment as people do, which means an unverified device isn't a minor gap. It's a direct operational and clinical risk.
This is where many teams get caught off guard. Non-human identities are still a major blind spot: only 5.7% of organizations have full visibility into their service accounts, and 79% have experienced secrets leaks, with 77% of those incidents causing tangible damage [1].
DIDs, verifiable credentials, and self-sovereign identity
A Decentralized Identifier (DID) is a unique, resolvable string that doesn't rely on a central registration authority. For HDOs, that gives patients and clinicians a portable way to prove who they are across systems.
Verifiable credentials (VCs) are cryptographically signed digital credentials, like a nursing license or insurance card. They live in a digital wallet and are presented straight to a verifier. The verifier checks the issuer's DID instead of going back to a central database each time.
Self-sovereign identity (SSI) brings those pieces together. People hold their own credentials and decide what they share.
In HDO workflows, issuance starts with a trusted authority, such as a state licensing board, credentialing body, or payer. That authority issues the credential to the holder's wallet. The holder then presents it, and the verifier resolves the issuer's DID on-chain to confirm validity. SSI still depends on trusted issuers - state boards, licensing bodies, and payers - to validate claims before a credential is accepted.
Once credentials can move across systems, the next job is making sure each verifier sees only what they need.
Selective disclosure and privacy-preserving verification
Not every check needs the whole record. A telehealth platform verifying insurance status doesn't need a patient's full name, address, or diagnosis history. Selective disclosure lets the holder share only the attributes needed for that interaction.
Zero-knowledge proofs (ZKPs) go a step further. A clinician can prove they have a valid medical license without exposing the full credential details. A patient can prove they meet an age threshold without sharing their date of birth.
That fits the minimum-necessary access model. And in practice, this is one of those decisions that's much easier to make early. Build for claim-level disclosure now; adding it later gets expensive.
These identity building blocks shape the reference architectures in the next section.
2. Reference Architectures for Blockchain Identity in HDO Environments
DIDs, verifiable credentials, and selective disclosure sound good on paper. But they only work in practice when they're tied to a trust architecture that an HDO can actually deploy.
At the core, that means one thing: keep identity anchors on-chain and keep PHI off-chain.
On-chain trust registries and off-chain PHI storage
The blockchain should handle only the pieces needed to verify trust, such as DIDs, credential schemas, public keys, and revocation status. PHI should stay where it already belongs: in EHRs, HIEs, or secure cloud storage.
Architectures such as the BDIMHS scheme follow this model. They use Hyperledger Indy for the ledger and Hyperledger Aries for agent and wallet infrastructure, while storing only public DIDs and credential definitions on-chain. [2]
DIDComm handles encrypted agent-to-agent messaging off-chain. [2]
That split matters. It limits what lands on the ledger and keeps clinical data out of places where it doesn't belong. It also sets up the next practical question: how these identity models fit day-to-day HDO workflows.
Patient and provider identity patterns with verifiable credentials
For patients, the model is simple in concept. A patient keeps verifiable credentials in a wallet and shares only the claims needed for a task like registration or check-in. The verifier can check the issuer's DID on-chain without pulling the patient's full record. Common credentials include government ID, medical power of attorney, and professional identity. [2]
Patient identity is mostly about consent and limited disclosure. Provider identity is different. It turns on licensing, status checks, and revocation.
Provider credentials need a tighter issuance and revocation process than patient credentials. Licenses, designations, and affiliations come from trusted authorities such as state licensing boards or medical boards, then get anchored to a permissioned ledger verified by the HDO. Revocation registries allow issuers to invalidate expired credentials without rewriting the ledger. [2]
You can think of it this way: a patient usually proves just enough about who they are, while a provider often has to prove they are still allowed to practice.
Integration with EHRs, HIEs, telehealth, OAuth 2.0, and OpenID Connect
The goal isn't to rip out existing IAM systems. It's to extend them.
In practice, HDOs can use agent middleware to connect EHRs and the blockchain trust layer through REST APIs and webhooks. [2] OAuth 2.0 and OpenID Connect can still handle authorization, with blockchain-verified credentials serving as the source of claims.
For telehealth, OpenID Connect and OAuth 2.0 can support session-scoped claims. Biometric binding can add holder assurance.
These patterns usually fall into three common architecture types:
| Feature | Patient SSI | Provider Credential Verification | Telehealth Identity Flow |
|---|---|---|---|
| Data Location | Off-chain (wallets/EHRs); DIDs on-chain | On-chain trust registries; PID off-chain | Federated IdPs; session-based claims |
| Interoperability | High (W3C-DID, VC, FHIR) | High (standardized PID schemas) | High (OIDC, OAuth 2.0, SAML) |
| Scalability | High (distributed, no central bottleneck) | Moderate (requires institutional trust anchors) | High (leverages existing IAM federation) |
| Governance | Patient-controlled | Regulatory/HDO-led, steward-managed ledger | Federated; trust framework-based |
| PHI Exposure | Minimal (selective disclosure/ZKP) | None (professional attributes only) | Low (encrypted assertions, session-scoped) |
These models can cut down data exposure, but they also bring governance and third-party risk management demands with them.
3. Security, Privacy, and Compliance Requirements
Those architecture choices still have to meet HIPAA, ONC, and zero trust requirements. Section 2 laid out the trust model. This section pressure-tests that model against regulation and day-to-day risk.
HIPAA, HITECH, and ONC considerations
HIPAA’s core demands - audit trails, access transparency, minimum necessary access, and patient access rights - line up with blockchain identity more closely than many HDO leaders expect.
Immutable on-chain transaction logs support HIPAA auditability by giving teams a tamper-proof record of who accessed what and when. [4][2]
HIPAA’s minimum necessary standard is where selective disclosure and Zero-Knowledge Proofs (ZKPs) start to matter. A ZKP lets a patient prove one claim - such as being over 18 - without showing the rest of their record. In plain English, the verification step itself limits what gets shared. [2]
The harder HIPAA issue is amendment requests. Immutability helps with audit logs, but it becomes a problem if PHI ends up on-chain. That’s why the safer design keeps corrections in off-chain wallets while the blockchain stores only DIDs, credential schemas, and revocation registries. [5][2][3]
ONC interoperability goals point the same way. W3C Verifiable Credentials and DIDs avoid centralized identity bottlenecks that weaken interoperability. They also make identity data machine-verifiable and portable across HDOs, HIEs, and telehealth platforms. [5]
The table below maps key compliance requirements to the design choices that address them:
| Compliance Requirement | Blockchain Identity Design Choice |
|---|---|
| HIPAA Audit Trails | Immutable on-chain transaction logs and access records [4][2] |
| HIPAA Minimum Necessary | Selective disclosure and Zero-Knowledge Proofs [2][3] |
| Patient Access Rights | Self-Sovereign Identity (SSI) wallets for user-centric control [5][2] |
| Right to Amend/Forget | Off-chain PHI storage with on-chain hashes or status pointers [5][3] |
| ONC Interoperability | W3C Verifiable Credentials and DID standards [5][2] |
| Breach Response | Credential revocation registries [2] |
Once compliance is mapped, the next problem is re-identification risk.
Zero trust controls and re-identification risk
Zero trust in blockchain identity isn’t optional. It has to be built into the design. Every interaction needs verification. Nothing gets assumed.
The main leftover threat is re-identification risk. Even if PHI stays off-chain, on-chain metadata - transaction patterns, timing, and DID correlations - can still be linked back to a person. The main safeguard is pairwise DIDs. A separate DID gets created for each holder-verifier relationship, so one identifier can’t follow a patient across many providers or services. [2] HDOs should also keep on-chain metadata to a minimum to cut down the attack surface for correlation.
Device trust follows the same rule. Medical devices that connect to blockchain identity infrastructure need continuous verification, along with dedicated device DIDs and encrypted communication channels that block unauthorized interception. [3]
Third-party risk and governance with Censinet
Zero trust controls only hold up if issuer, wallet, and vendor risk are managed all the time.
Blockchain identity programs don’t remove third-party risk. They move it around. Instead of running one centralized identity repository, HDOs now manage a network of issuers, wallet providers, and ledger stewards. Each one brings PHI exposure risk, integration security risk, and supply chain security challenges.
Use Censinet RiskOps™ to manage issuer, wallet, and vendor risk across the identity stack, including third-party and enterprise risk assessments, cybersecurity benchmarking, and collaborative risk management.
One governance gap shows up again and again in blockchain identity deployments: vendor offboarding. Research shows that only 20% of organizations have formal processes for revoking API keys when a vendor relationship ends. [1] Decentralized identity can help close that gap at the technical level. HDOs can issue temporary, time-bound verifiable credentials to third-party vendors and revoke them automatically when a contract ends or a policy is violated [4][2] - but the governance process still has to be defined and enforced. Censinet RiskOps™ supports that review cycle with structured risk management workflows.
4. Implementation Roadmap for HDOs
With the trust model set, the next step is moving from design into production in controlled phases. A 90/180/360-day rollout helps cut risk while showing value early. Start with the narrowest workflow possible - one that tests identity, revocation, and off-chain storage from end to end.
Assess identity gaps and prioritize high-value use cases
Before picking any stack, map where trust breaks down today. In HDOs, common weak spots show up in patient registration, clinician onboarding, vendor access, consent management, provider directory accuracy, and audit trail integrity for Information Blocking investigations.
Information Blocking penalties can reach $1,000,000 per violation [6], which makes tamper-evident audit trails both a business issue and a compliance issue. The best place to start is usually not shared clinical data. It’s the workflows where shared identity causes the most friction.
Early use cases tend to work best when more than one party has to agree on the same claim, such as:
- consent attestation using W3C Verifiable Credentials mapped to HL7 FHIR Consent
- ledger-backed provider directories
- prior authorization evidence for PAS/CRD/DTR workflows
- tamper-evident audit indexes based on IHE ATNA/BALP patterns
The Synaptic Health Alliance used a shared provider-data ledger and reported less rework, with MultiPlan citing a 500% annual ROI [6].
Choose technology components and run a safe pilot
Once the use case is set, choose only the parts needed to prove the trust model under production-like conditions. For regulated B2B workflows, Hyperledger Fabric 2.5 LTS supports private data collections and secure channels. If the HDO needs EVM compatibility or public-anchor patterns, Hyperledger Besu with Tessera is the other option [6][2]. Pick the one that lines up with the pilot’s interoperability path and governance model.
Keep clinical data in secure off-chain repositories. Put only salted hashes and metadata on the ledger [6][7]. Use W3C Verifiable Credentials 2.0 and DIDs, and connect apps through SMART on FHIR v2 apps [6][2].
For the pilot, keep scope tight. One health system and one payer is enough. A narrow target - like notarizing ADT messages or lab AuditEvents - makes it easier to measure success without turning the pilot into a sprawling program.
Manage credential lifecycle, monitoring, and risk review
A blockchain identity program needs clear ownership for issuance, verification, and revocation before go-live. Revocation registries let teams invalidate credentials without exposing private data [2]. Key protection should rely on hardware-backed modules and NIST-approved encryption with scheduled rotation [7].
Monitoring should sit inside identity operations, not off to the side as a separate security task. HDOs should keep a live threat model, a Data Protection Impact Assessment (DPIA), and a runbook for QHIN outages or EHR updates [6]. Risk reviews should also track USCDI v3 and CMS FHIR API deadlines [6]. At each phase gate, reassess third-party and enterprise risk.
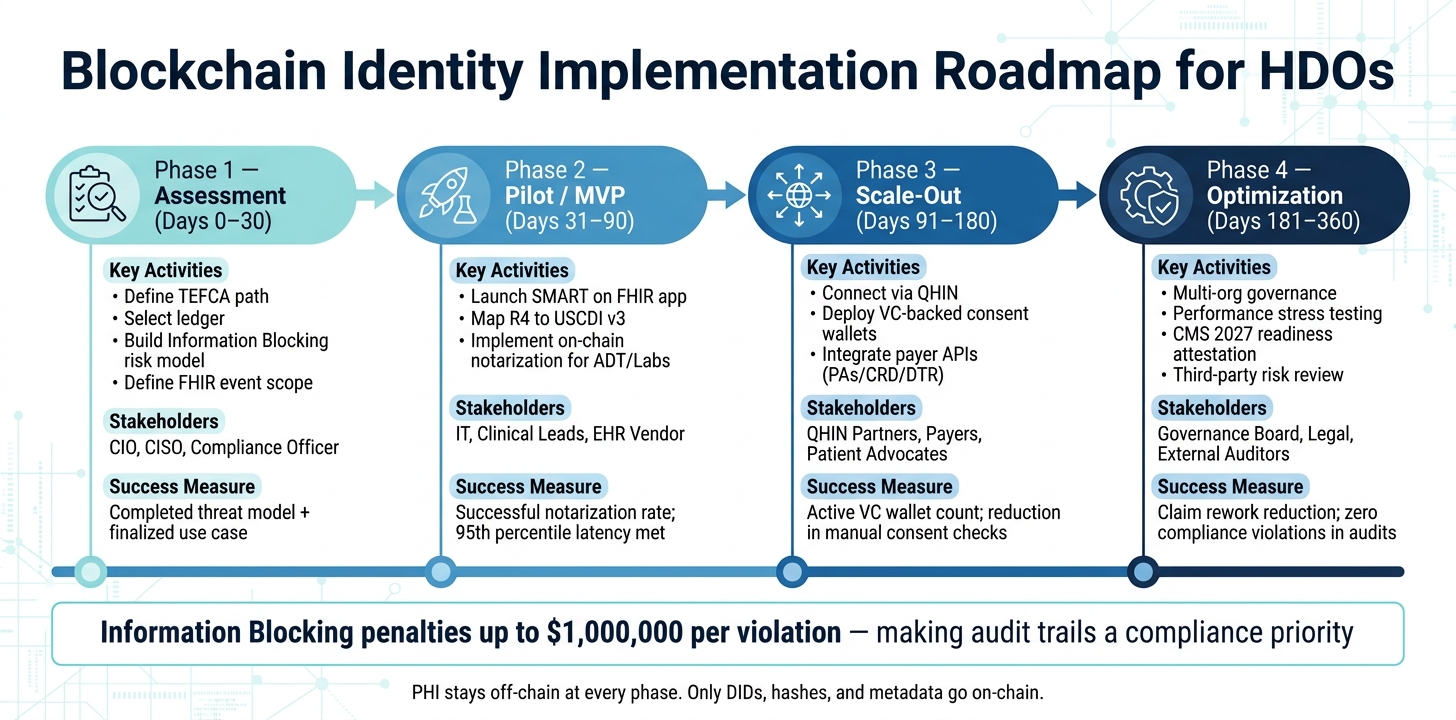
The roadmap below ties each phase to one operating choice: what to trust, what to store, and what to verify.
| Phase | Timeline | Key Activities | Stakeholders | Success Measures |
|---|---|---|---|---|
| Assessment | Days 0–30 | Define TEFCA path; select ledger; build Information Blocking risk model; define FHIR event scope | CIO, CISO, Compliance Officer | Completed threat model; finalized use case |
| Pilot (MVP) | Days 31–90 | Launch SMART on FHIR app; map R4 to USCDI v3; implement on-chain notarization for ADT/Labs | IT, Clinical Leads, EHR Vendor | Successful notarization rate; 95th percentile latency met |
| Scale-Out | Days 91–180 | Connect via QHIN; deploy VC-backed consent wallets; integrate payer APIs (PAS/CRD/DTR) | QHIN Partners, Payers, Patient Advocates | Active VC wallet count; reduction in manual consent checks |
| Optimization | Days 181–360 | Multi-org governance; performance stress testing; CMS 2027 readiness attestation; third-party risk review | Governance Board, Legal, External Auditors | Claim rework reduction; zero compliance violations in audits |
Conclusion: What HDOs Should Take Forward
Blockchain should be the trust layer, not the place where PHI lives. Keep PHI off-chain, and store only hashes, metadata, and DIDs on the ledger [7][3].
DIDs, verifiable credentials, selective disclosure, and zero-knowledge proofs give HDOs a way to verify identity claims without sharing more data than needed [2][3]. That said, privacy-preserving identity rises or falls on governance. If there are no clear rules for how credentials are issued, used, and revoked, the model can break down fast.
Durable deployments depend on a few basics done well: permissioned access, clear BAAs for participants, enforced minimum-necessary rules, and a defined credential lifecycle for issuance, rotation, and revocation [7][2].
For third-party and enterprise risk reviews, Censinet RiskOps™ supports governance across vendors, devices, and clinical applications.
Start with a narrow use case. Prove the trust model end to end. Then scale.
FAQs
Why shouldn't PHI be stored on a blockchain?
Storing raw PHI on a blockchain is usually a bad idea. It increases exposure, makes key rotation more difficult, and clashes with needs like data correction.
Here’s the core issue: blockchain data is often immutable and copied across many nodes. That means if sensitive information is written on-chain, it can create privacy and regulatory risk fast. A better approach is to keep PHI off-chain and put only hashes or metadata on the blockchain.
How do DIDs and verifiable credentials fit into our current IAM stack?
DIDs and verifiable credentials move identity management away from central control and toward a self-sovereign model, where people control their own identity data.
In your IAM stack, DIDs work as user-controlled identifiers. Verifiable credentials are digital, cryptographically verifiable versions of documents.
Access flows through three roles:
- Issuers, who create and sign credentials
- Holders, who store and present them
- Verifiers, who check that the credentials are valid
To support privacy and compliance, sensitive PHI stays off-chain.
What’s the best first use case for an HDO pilot?
A strong first use case for an HDO pilot is a workflow that checks one claim at a time - like insurance eligibility, patient age, or portal access - without exposing full protected health information (PHI).
That fits HIPAA’s minimum necessary standard. Instead of storing raw data, the system can prove identity claims with cryptographic credentials. For HDOs, that creates a focused, lower-risk way to test decentralized identity.
