Rural healthcare’s AI problem is simple: tools are getting used before anyone sets clear rules for them. In many rural hospitals and clinics, AI is now part of charting, diagnosis support, and patient messaging. But many teams still lack a full inventory, named owners, vendor checks, and routine review.
Here’s the short version:
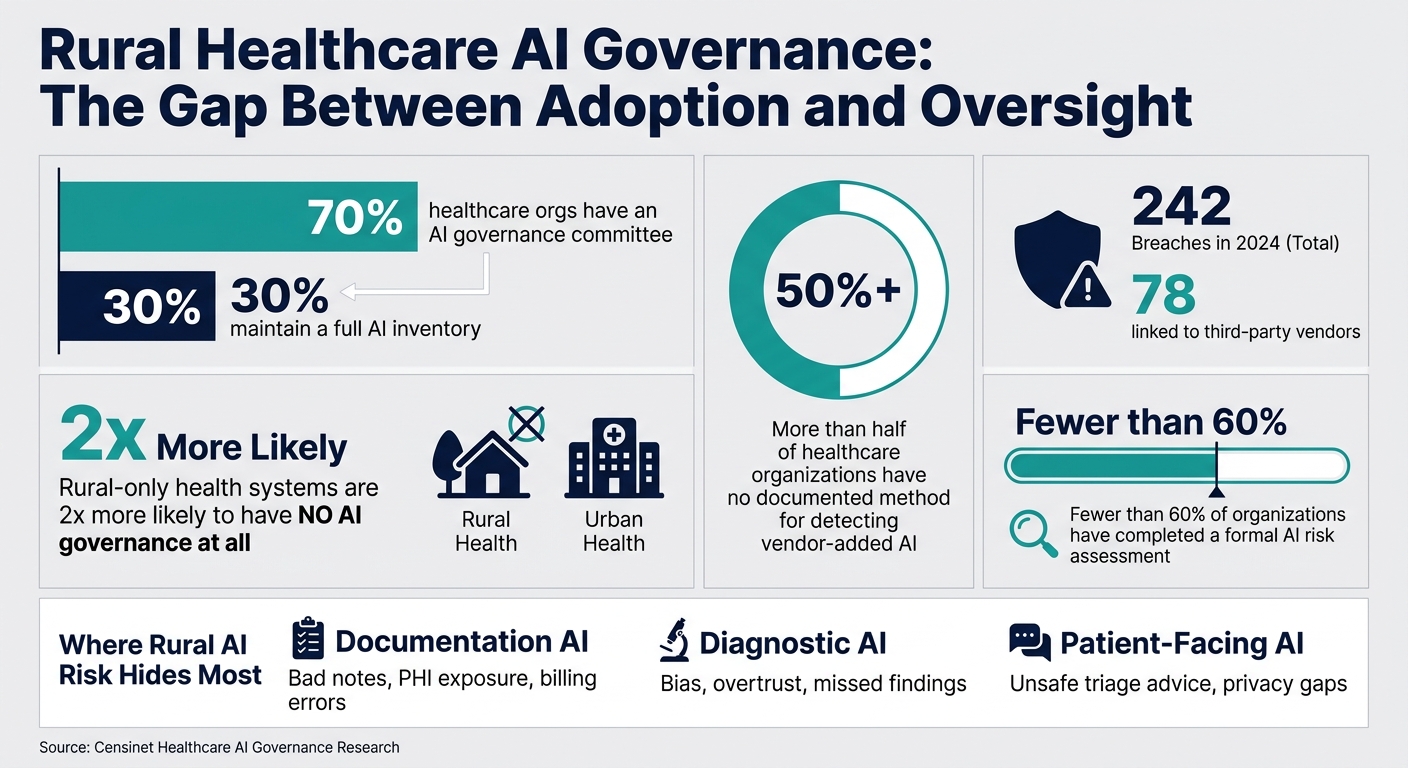
- 70% of healthcare groups have an AI governance committee, but only 30% keep a full AI inventory.
- Rural-only systems are 2x more likely to have no AI governance at all.
- 50%+ of healthcare groups have no written way to detect AI added through vendor updates.
- Third-party AI risk is already a problem, with 242 healthcare breaches in 2024, including 78 linked to third parties.
What this means for me is clear: if I run a rural provider, I can’t treat AI as just another software feature. I need to know which tools use AI, what data they touch, who owns each one, and how issues get escalated.
The article’s main point is straightforward:
- Hidden vendor AI can create patient safety, privacy, billing, and security risk
- Small teams often struggle because AI review gets added to jobs people already have
- Weak ownership means incidents can sit in limbo
- A simple model works best: inventory, risk tiers, vendor review, named owners, and monitoring
If I had to boil it down to one line, it would be this: AI in rural care needs basic control before it needs more adoption.
A few areas stand out most:
- Documentation AI: may draft wrong notes or send PHI to outside services
- Diagnostic AI: may miss local population patterns or be trusted too much
- Patient-facing AI: may give unsafe triage advice when distance and access matter
| Area | Main Risk | What to put in place |
|---|---|---|
| Documentation AI | Bad notes, PHI exposure, billing errors | Note audits, clinician sign-off, vendor data checks |
| Diagnostic AI | Bias, overtrust, missed findings | Local testing, use limits, review rules |
| Patient-facing AI | Unsafe advice, privacy gaps | Escalation rules, consent language, channel review |
The fix is not a big new program. It’s a short, repeatable process that a small rural team can keep up with over time.
Rural Healthcare AI Governance: Key Stats & Risk Gaps
Jorie Tech Talks: Episode 15 "AI and the Future of Rural Healthcare with Heritage Health"
sbb-itb-535baee
How unguided AI creates clinical, cyber, and compliance risk
AI risk in rural healthcare often starts in a pretty ordinary way. A vendor pushes an update. A feature turns on by default. Suddenly, AI is helping draft clinical notes, suggesting diagnoses, or replying to patient messages before anyone has stopped to check how it works in practice.
That’s the core issue: the tool shows up before the review process does. And when there’s no formal review in place, problems stay out of sight until a bad note, a poor recommendation, or a privacy incident forces people to pay attention.
How clinical documentation, diagnostic, and patient-facing AI each fail differently
These tools don’t fail in the same way. But they usually break for the same reason: no one is watching how the AI is being used day to day.
A clinical documentation tool might auto-complete a care plan that assumes a patient can follow up by telehealth within 48 hours or get services that simply don’t exist nearby. On paper, the note looks fine. In practice, it misstates the actual plan and can skew quality metrics.
A diagnostic support tool has a different problem. If it was trained mostly on urban academic data, it may underrate cardiovascular risk in a rural population with higher smoking rates and more occupational exposure. It may also produce high-confidence output that clinicians trust too much.
Patient-facing AI can fail in a more direct way. A chatbot might tell a person with chest pain to see their doctor in 3 days, without any sense that the nearest emergency department could be hours away. That kind of advice isn’t just off. It can be dangerous.
| AI Tool Type | Typical Benefits for Rural Providers | Key Cybersecurity and Governance Risks | Oversight Needed |
|---|---|---|---|
| Clinical documentation AI (scribes, summarization, coding support) | Cuts documentation burden and supports coding. | PHI transmitted to external cloud services; unclear data retention and training use of PHI; hallucinated content affecting billing and clinical decisions. | Vendor security and privacy review; BAA and data-use limits; sampling audits of AI-generated notes; clinician review and attestation policy. |
| Diagnostic support AI (imaging, risk scores, decision support) | Supplements limited specialist access; flags high-risk patients earlier. | Bias from non-representative training data; clinicians overtrust results; unclear accountability for AI-influenced diagnoses. | Local validation against rural population data; documented limits of use; defined roles for reviewing and acting on AI alerts. |
| Patient-facing AI (chatbots, virtual assistants, symptom checkers) | Extends access outside business hours; reduces phone burden. | Unsafe triage guidance; lack of AI transparency to users; consent and data-use ambiguity; PHI exposure via insecure channels. | Clear disclaimers and consent messaging; automatic escalation for high-risk symptoms; privacy and security assessment of communication channels; periodic log review. |
What rural organizations miss in vendor-delivered AI
The bigger problem is often the AI hiding inside tools the organization already trusts. EHRs, imaging platforms, and patient communication systems now ship with AI features built into normal upgrades - auto-coding suggestions, imaging triage flags, predictive scheduling, and more. They don’t always arrive with a big label that says this is AI.
Because these features come in as product add-ons instead of brand-new programs, they often skip governance review. That leaves a blind spot. Across healthcare, 38% of organizations either split AI risk responsibility across several groups without clear escalation paths or have not defined ownership at all [1].
There’s also the vendor chain behind the vendor. AI features may depend on cloud platforms, annotation services, and model hosts - downstream vendors and subprocessors. A rural provider may have a BAA with the main vendor and still have little to no visibility into where PHI goes after that. If a subprocessor has a security or privacy incident, patient data can still be exposed. Healthcare saw 242 breaches in 2024, including 78 tied to third parties [2]. As more AI features get folded into vendor platforms, that tracking job gets harder.
Why accountability breaks down when no one owns the AI decision path
Once AI decisions are spread across clinical, IT, procurement, and compliance, ownership gets fuzzy fast. Clinical leaders may approve a tool because it fits the workflow. IT may turn on features for compatibility. Procurement may sign based on cost. Compliance may review the BAA but never dig into what the AI is actually doing.
So the full decision path exists, but no single person owns it.
That becomes a problem the minute something fails. A chatbot gives unsafe triage advice. A diagnostic tool misses a finding. A documentation tool drafts a note that leads to a billing audit. At that point, frontline staff need a clear answer on who handles the fix. Too often, they don’t get one.
In small rural organizations, this gets even messier because one person may cover IT, privacy, and vendor management at the same time. In that setup, a missing escalation path isn’t just an admin gap. It becomes a direct patient safety and compliance risk.
The root causes behind the governance problem
Rural AI governance tends to break down when three things collide: limited staff, weak data controls, and fuzzy ownership around vendor-built AI. It’s not usually one big mistake. It’s the same pattern showing up again and again.
Limited staffing and expertise make review inconsistent
In many rural settings, AI governance doesn’t belong to a full-time team. It gets added to someone’s already packed job. That means AI model review, log auditing, and policy upkeep all compete with other urgent work. Something usually slips.
"Rural health systems face the same cyber threats and the same pressure to adopt AI as the largest systems in the country, but without the same budgets or the same bench depth." - Brian Sterud, VP and CIO, Faith Regional Health Services [1]
Once that workload piles up, AI review becomes irregular and reactive. Teams step in when there’s a problem instead of checking systems in a steady, routine way. And when review is manual and ad hoc, AI use can drift outside normal controls.
That’s how checkbox governance takes hold. A committee gets formed. A charter gets written. On paper, it looks like progress. But the day-to-day work - keeping an AI inventory up to date, watching vendor activity, and assigning plain ownership - doesn’t fully happen.
"Healthcare has built the governance scaffolding for AI, but the operational muscle - inventory, asset management, detection methods, and clear accountability - is not keeping pace with adoption." - Ed Gaudet, CEO, Censinet [1]
And even if staff do catch a problem, weak data controls can still let unsafe AI move forward.
Data governance gaps weaken safe and compliant AI use
A Business Associate Agreement can help, but it doesn’t solve everything. If a vendor adds a new AI feature later, that feature may fall outside the original BAA. So even when a rural provider thinks the paperwork is covered, patient data may be processed in a new way that was never reviewed. That can create HIPAA risk without anyone noticing right away.
There’s another issue: model drift. That happens when an AI system gets less accurate as local data changes over time. It’s a quiet problem. If no one is checking performance on a regular basis - and if audit logs are weak or missing - drift can sit there unnoticed.
More than 50% of healthcare organizations have no documented method for detecting when vendors add AI into existing products [1]. That’s a big gap. It means vendor AI can slip past the normal review workflow and start handling sensitive data with little visibility.
Common rural barriers mapped to minimum governance controls
The barriers below line up with the minimum controls rural teams need.
| Barrier | Impact on AI Safety and Compliance | Minimum Governance Control Needed |
|---|---|---|
| Limited staffing and expertise | Inconsistent review of logs and model behavior. | Named AI risk owner; automated AI inventory and centralized RiskOps platform. |
| Vendor-embedded AI | PHI is processed by unvetted algorithms; existing BAAs may not cover new AI features. | Continuous vendor data access monitoring and inventory; BAA update requirements. |
| Data governance gaps | Bias in underrepresented populations; lack of audit trails for HIPAA. | Local performance validation and centralized audit logging; limit data use to the approved purpose. |
| Fragmented ownership | No clear escalation path during an AI-related incident or compliance violation. | Assign one escalation owner and one backup owner; shared audit logs. |
In practice, the fixes are pretty basic. Keep a simple inventory. Put one person in charge, plus a backup. Monitor vendor activity and log use in one place. Those steps won’t solve every AI governance issue, but they do close many of the most common gaps.
A practical AI governance model rural providers can apply now
Rural teams don't need a big AI program. They need a process they can repeat: inventory, tier, review, and monitor. That's the part that matters.
For small teams, simple wins. Start by listing what you have and who owns it. Then add risk tiers, review steps, and basic monitoring.
Build an AI inventory and assign simple risk tiers
The first step is plain but easy to miss: know what AI is already in your environment. Fewer than 60% of organizations have done a formal AI risk assessment [3]. That gap matters because AI doesn't always arrive with a big announcement. It often shows up through vendor updates, department purchases, or pilot projects that never go through a formal review. That's especially common with AI built into EHR, imaging, and patient communication tools.
An AI inventory is simply a running list of every AI tool in use. That includes embedded features, pilot projects, and workflow automation. For each tool, note:
- data used
- PHI exposure
- approved uses
Once you have that list, give each tool a simple risk tier based on what it touches and how it's used:
- High: AI that affects clinical decisions or handles PHI
- Medium: AI used in workflows with human review
- Low: Administrative AI with little patient data
This kind of tiering helps a small team spend time where it counts. A scheduling tool does not need the same level of review as a tool that affects clinical decisions. Matching review effort to actual consequence keeps governance workable for a two- or three-person IT team.
Add vendor review checkpoints, named owners, and monitoring controls
After the inventory is in place, each tier needs a short review path. For higher-risk tools, that means asking vendors AI-specific questions during contracting, not just sending the usual security questionnaire.
Ask them directly: Does this product use AI or machine learning? What data does it process? How are model updates handled?
You also need the right people in the room. Review should include clinical, technology, legal, and operations input. And every AI tool should have two named owners:
- Business owner: approves use and escalates issues
- Technical owner: manages access, monitoring, and vendor contact
This two-owner setup closes the accountability gap without forcing a rural provider to build a separate AI governance team.
Monitoring matters too. Watch for performance drift. Protect AI-related data with role-based access, multi-factor authentication, and encryption. Those controls help surface clinical and compliance problems early. It also helps to disclose which tasks are automated and how outputs are reviewed.
Policy should stay short and direct. Spell out what AI is approved for, which tasks need human review before action is taken, and which use cases are off-limits. In rural care settings, AI should support staff, not replace human judgment or the patient relationship. The point is to create a repeatable review path, not hand out a one-time approval and move on.
Ad hoc AI adoption vs. governed AI adoption
The gap between ad hoc and governed AI isn't about bigger budgets or more staff. It's about having a repeatable process. Here's what that looks like in day-to-day practice.
| Dimension | Ad Hoc AI Adoption | Governed AI Adoption |
|---|---|---|
| Safety & Quality | Unmonitored performance drift and potential clinical errors. | Regular audits, spot-checks for output quality, and human-in-the-loop controls. |
| Compliance | Fragmented adherence to HIPAA and evolving state/federal guidelines. | Centralized risk tracking and automated compliance monitoring. |
| Vendor Visibility | Shadow IT and unvetted AI features embedded in existing software. | Formal vendor review checkpoints and named technical/business owners. |
| Staff Trust | Skepticism and fear of replacement or increased workload. | Transparency, training, and AI tools designed to reduce administrative burden. |
When inventory, ownership, and monitoring sit inside one workflow, governance is much easier to keep up to date as AI use grows.
How Censinet helps rural providers put AI governance into practice
That approach only works if inventory, review, and ownership sit inside one workflow. For rural providers, AI governance has to cut manual work while still keeping people in charge of the final decision.
Using Censinet RiskOps to centralize AI inventory, controls, and ownership
Censinet RiskOps can serve as the system of record for AI-enabled vendors, applications, and medical devices. Instead of juggling spreadsheets and email threads, rural teams can keep each item tied to its contracts, HIPAA-compliant risk assessments, security artifacts, technical integration details, and named owners in one place.
That makes day-to-day oversight much easier. Leaders can quickly see:
- which AI tools touch ePHI
- which ones have open remediation tasks
- which ones still need formal review
Faith Regional Health Services, a rural provider in northeast Nebraska, moved from manual vendor questionnaires to Censinet's automated platform. That shift gave the organization documented risk acceptance where it had not existed before:
"One of the biggest takeaways has been clearly defining risk acceptance. In the past, stakeholders didn't always realize that by not funding security initiatives, they were implicitly accepting risk. Censinet has helped us bring that conversation to the forefront." - Brian Sterud, CIO/CISO, Faith Regional Health Services [4]
Using Censinet AI and Censinet AITM to scale review without losing human control
Once the inventory is in one place, the next choke point is vendor review. And that's where many rural IT teams hit the wall. Vendor documents take time they simply don't have.
Censinet AITM ingests vendor documentation and produces risk-focused summaries that flag data flows, encryption, subprocessors, and fourth parties. In plain terms, it can surface cloud hosting, subprocessor, and data-flow issues before go-live.
Censinet AI takes on routing and classification tasks that might otherwise land on an already stretched compliance lead. It can:
- suggest a risk tier for a new vendor
- draft a remediation task list based on detected gaps
- route the assessment to IT, compliance, or clinical leadership using configurable rules
A person still makes the final call. That person confirms the tier, approves or adjusts remediation tasks, and decides whether a gap is a blocker or an accepted risk with compensating controls. In rural settings, that human review matters even more, because staffing limits shape every risk decision.
Conclusion: AI governance must keep pace with AI adoption
The goal isn't more process for the sake of process. It's governance a small team can repeat and maintain.
AI is showing up faster than the oversight structures many providers need to manage it safely. Inventories, risk tiers, vendor checkpoints, named owners, and monitoring controls help close that gap. And they don't require a large team to function. Rural providers can roll out these controls in stages, starting with the highest-risk AI tools and expanding from there as AI adoption grows.
FAQs
How can a rural provider find hidden AI in vendor updates?
Keep a complete AI inventory of every third-party tool you use. That includes obvious AI products, but also AI features tucked inside systems you already rely on, like EHRs, billing platforms, and other vendor software.
Then go a step further: ask vendors direct, AI-specific questions. Get contract language that requires notice when they make material changes. And don’t treat approval as a one-and-done task. Track for model drift and watch for use that starts to spill past the approved purpose.
Who should own AI governance in a small rural health system?
AI governance works best when a multidisciplinary committee owns it and has clear authority to make decisions.
That committee shouldn’t be vague or ceremonial. It needs the power to set direction, resolve disputes, and make calls when tradeoffs come up.
It also helps to assign two main owners:
- A clinical lead - such as the CMO or Medical Director - to oversee patient safety
- A technical lead - such as the CIO or CISO - to oversee performance, security, and infrastructure
On top of that, a senior executive who reports to the CEO should coordinate the work and back it with leadership support.
What is the minimum AI governance process a rural clinic needs?
A rural clinic does not need a big AI program. It needs a lean process that flags the highest-risk issues first, using the staff and budget it already has.
At a minimum, that means:
- Keep an AI inventory
- Assign one owner per tool
- Confirm a BAA before any tool handles PHI
- Test each tool on 20 to 50 local cases before launch
- Require human review for high-risk outputs
- Set written rules to pause or roll back a tool if safety or performance problems show up
That’s the core idea: start small, stay clear-eyed, and put guardrails around the places where mistakes can hurt patients or disrupt care.
