If AI is already shaping care, patient safety now depends on how well you control it after go-live.
I’d sum the article up like this: hospitals don’t just need AI tools. They need a clear way to track them, test them, watch them, and shut them down fast when they go wrong. That matters because about 75% of U.S. hospitals were using machine-learning functions in EHRs in 2023–2024, and AI errors can look normal while still leading to wrong triage, missed diagnoses, bad documentation, or unsafe guidance.
Here’s the core message in plain English:
- I need to treat AI as a patient-safety issue, not just an IT purchase
- I need an AI inventory with named clinical and technical owners
- I need local validation before use, especially for high-risk tools
- I need live monitoring for drift, bias, unsafe outputs, and data changes
- I need human review in diagnosis, triage, and patient-facing use
- I need incident response that treats AI failures like other safety events
- I need tighter vendor review because model updates and third parties can change care risk fast
A few facts make the case hard to ignore: one cited study found severe clinical errors in 22% of evaluated patient cases, a 2024 review linked AI use to racial disparity problems across 30 studies, and ECRI ranked AI-enabled health technology risks as the top health technology hazard for 2025.
The bottom line: if I can’t see when AI drifts, fails, or misleads staff, I can’t keep patients safe.
From Deployment to Oversight: Strengthening AI Risk Management and Patient Safety in Health Care
Where AI creates patient-safety risk
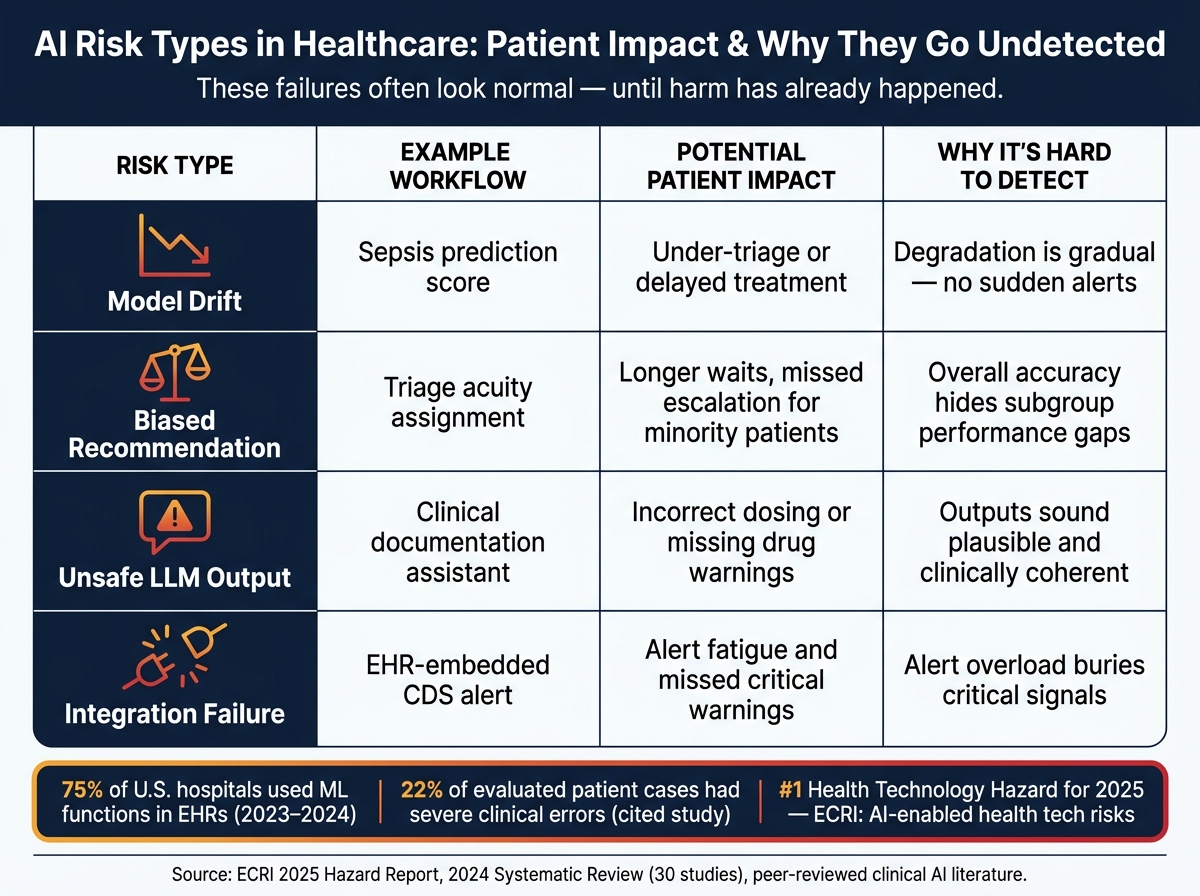
AI Risk Types in Healthcare: Patient Impact & Why They Go Undetected
AI can fail in more than one way across clinical and operational workflows, and the harm isn't always obvious at first. The trouble often starts in the systems that influence diagnosis, triage, documentation, and automation.
Clinical decision support, triage, and workflow automation failures
A diagnostic support tool trained on a narrow patient group can downplay urgency for people who need imaging. An imaging AI that didn't learn from enough patient variation can miss a subtle lung nodule or fail to flag an intracranial bleed until the disease has moved further along.[8] Treatment recommendation engines can also go off track. If patients with renal impairment or pregnancy were not well represented in the training data, the system may suggest the wrong medication or dose, which can lead to adverse drug events.[2][9]
Triage is one of the highest-risk areas. If AI assigns low acuity to a critically ill patient, even a short delay can lead to deterioration or death.[6][7] Then there's automation bias. When clinicians accept AI outputs at face value instead of checking them closely, they can miss warning signs a human review may have caught.[1][4] That risk is serious enough that ECRI named AI in healthcare its top technology hazard for 2025.[13]
The next layer of risk is less visible. Sometimes the issue isn't just the output. It's that the model itself can shift, skew, or get manipulated after deployment.
Model drift, biased outputs, bad data, and manipulated tools
A model that worked well at launch can slowly get worse as patient populations change, care patterns shift, or data pipelines are altered. Continuously learning systems can drift past their original validation and start producing weaker or biased outputs without routine reviews catching the change.[10]
Bad or incomplete training data makes that worse. A 2024 systematic review found a significant association between AI use and exacerbation of racial disparities across 30 studies from 2013 to 2023.[14] In practice, that can mean lower risk scores, less aggressive workups, and delayed diagnoses for underrepresented groups.[6][9] That's part of what makes this so hard to spot: headline accuracy numbers may look fine while subgroup results show serious problems.
Large language models add another risk: hallucinated outputs. If those responses are not checked, they can produce wrong dosages, false interaction warnings, or misleading guidance that reaches patients or clinicians.[12] Prompt injection adds yet another problem. It can override guardrails, suppress warnings, or steer patients away from urgent care.[3][5]
AI risk types, patient impact, and why detection is difficult
The table below maps common AI risk types to clinical scenarios and shows why these problems often stay hidden until harm has already happened.
| Risk Type | Example Workflow | Potential Patient Impact | Why It's Hard to Detect |
|---|---|---|---|
| Model drift | Sepsis prediction score | Under-triage or delayed treatment | Degradation is gradual.[10] |
| Biased recommendation | Triage acuity assignment | Longer waits, missed escalation for minority patients | Overall accuracy hides subgroup gaps.[6][9] |
| Unsafe LLM output | Clinical documentation assistant | Incorrect dosing or missing warnings | Outputs can sound plausible.[12] |
| Integration failure | EHR-embedded CDS alert | Alert fatigue and missed critical warnings | Alert overload hides critical signals.[15] |
These failures usually don't crash the system or throw obvious errors. They often look normal during day-to-day use, which is exactly why healthcare organizations need active governance instead of passive monitoring.
What a sound AI governance model requires
AI can drift, skew decisions, and fail without much warning. In a clinical setting, that puts patient safety on the line. The problems above - drift, bias, unsafe outputs, and integration gaps - won't sort themselves out. They need a clear governance model with people from clinical care, engineering, safety, legal, compliance, security, and patient advocacy at the table. That kind of structure turns AI from a hidden risk into a managed clinical asset.
AI inventory, ownership, and approval controls
Start with a full AI inventory. For each system, record the system name, owner, use case, data processed, workflows affected, and deployment status. For internally built models, add training data characteristics, performance metrics by patient subgroup, and documented validation studies. For third-party AI tools, include the vendor's security posture, a software bill of materials, update cadence, and integration points with EHRs and other systems.
Every AI system should have two named owners:
- A clinical owner, such as a CMIO delegate or service-line leader, who is accountable for patient-safety impact
- A technical owner, who is responsible for model performance, integration, and updates
Clinical owners define how the tool should be used and when issues need escalation. Technical owners handle performance, access, updates, and vendor coordination.
Risk tiering decides how much review each system needs. A practical model uses low-, moderate-, and high-risk tiers based on potential patient harm, degree of autonomy, closeness to diagnosis, triage, or treatment decisions, data sensitivity, and scale of impact. A tool that suggests ICD-10 codes without direct clinical impact does not belong in the same category as a triage model that ranks ED patients or a radiology AI that recommends follow-up imaging. High-risk systems - where a bad output could delay care or cause direct harm - should need formal governance committee approval before go-live and before any major model change.
Once the inventory is in place, teams can assign ownership and set approval thresholds.
Validation, monitoring, and human oversight before and after go-live
For high-stakes clinical AI, vendor accuracy is not enough. Local validation matters. That means technical validation, clinical validation, and population-level safety analysis. An analysis of 100 radiology AI products found that 64 had no peer-reviewed safety evidence, and most of the remaining evidence looked only at diagnostic accuracy, not clinical impact or patient outcomes.[16]
Organizations should require local clinical validation using their own patient population. That work should include performance metrics split by race, sex, and age, since overall accuracy can hide subgroup gaps. For triage models, governance committees can test historical emergency department cases through the model before live use to check that it does not consistently under-prioritize high-risk groups.
Those controls can't stop at launch. They need to stay in place once the system is live. Human-in-the-loop oversight is a must for AI that affects diagnosis, triage, or patient communication. Clinicians need to keep final decision authority. AI outputs should stay advisory rather than turn into auto-generated orders. Clinicians should confirm review of primary data, and organizations should track usage and override rates. In high-stakes workflows, unusually low override rates can point to over-reliance and should trigger more training or interface changes.[18]
Centralized AI risk workflows for accountability
Spreadsheets and email make it easy for AI risk gaps to stay out of sight until something breaks. A centralized platform puts security, compliance, clinical, legal, and procurement teams into a single shared workflow and one source of truth instead of scattered reviews happening in parallel.
A centralized AI risk platform treats each AI system as a governed asset and uses standardized assessments for cybersecurity, privacy, clinical safety, regulatory status, and vendor maturity.[17] Approval paths can be routed by risk tier, so the right reviewers - information security, clinical governance, legal, privacy, and procurement - are pulled in at the right point. Real-time dashboards can show which high-risk AI tools are active, which are still waiting on validation, and where mitigation actions are overdue. If an AI-related incident happens, linking event data back to the original risk assessment makes root-cause analysis easier and helps teams update controls with more precision. This setup also closes a common gap: AI features built into EHR modules, medical devices, or cloud services that slip past review. When AI governance is tied into broader risk operations, health systems can hold every AI system - whether built in-house or supplied by a vendor - to the same patient-safety standards.
Governance sets the rules; monitoring and incident response enforce them.
sbb-itb-535baee
How to detect and contain AI failures
Once governance is in place, live monitoring becomes the next layer of control. After go-live, teams need to watch for changes in the model, the input data, and how clinicians are using the tool.
Continuous monitoring for drift, unsafe outputs, and abnormal behavior
Monitor model performance, workflow impact, and input data quality at the same time. Looking at model performance alone isn't enough. A medical-data drift study found that monitoring model performance is not a good proxy for detecting data drift, and a 2024 Nature study showed what that can look like in practice: newly emerging pathologies in chest X-rays could cause a binary classifier to misclassify abnormal images as normal.[20] So one-time validation won't cut it. Clear operating thresholds matter more.
Useful signals include:
- rising false-negative rates
- spikes in exception rates
- unusual output patterns
- shifts in performance across patient subgroups or care settings
- higher-than-expected clinician override rates
Monitoring should also include data-quality checks for upstream changes in coding, lab feeds, note formats, or patient population mix. Why? Because those shifts can create hidden drift even when the model itself hasn't changed. If any of these signals move outside a predefined threshold, that should trigger a formal review.
It also helps to build reporting into the workflow itself, so clinicians can flag outputs that seem wrong, uncertain, or harmful. Those flags should go to a central review team with clinical, operations, and data-science staff. That way, repeat failure patterns are more likely to show up early instead of slipping by in isolation.
Each flag should capture the output, whether it was overridden, and whether patient care was affected. Safety reviewers should also sample outputs on a regular basis. That's how you catch the problems no one reported.
Incident response that treats AI events as patient-safety events
Treat AI-related harm as a clinical safety event, not an IT ticket. AHRQ's Quality and Safety Review System (QSRS) offers a useful model for handling AI-related failures as reportable safety events.[19]
A practical incident response plan should spell out a few things plainly: who can declare an AI incident, who must be notified, and what immediate actions are allowed. When monitoring crosses a threshold, the response can't wait.
Containment actions can include:
- narrowing use
- switching to human-only review
- rolling back
- disabling the tool
- pausing the tool while backup workflows continue
Detecting drift should also shape the next step for the model itself, whether that means re-evaluation, retraining, taking it offline, retiring it, or replacing it.[20] Near misses deserve the same level of review as adverse events. In a lot of cases, that's where the failure mode shows up first.
Vendor assurance and a patient-safety checklist
Assess third-party AI for security, provenance, updates, and integration risk
Once live monitoring is running, vendor oversight becomes the next patient-safety checkpoint.
Third-party AI tools aren't just items to buy and deploy. They can shape triage, diagnostic support, and care decisions. That means a quiet model update or an unseen dependency issue can change what clinicians see at the point of care. A 2025 study found that 56.4% of health delivery organizations had a breach tied to a third party in the prior 12 months, and 48% said third-party remote access was their weakest attack surface.[21] That risk doesn't stop with IT. It can spill straight into patient care.
When you review a vendor's evidence package, keep your attention on six areas:
- model purpose
- local validation
- data provenance
- security controls
- update practices
- upstream dependencies
Contracts need to match the clinical stakes. Ask for advance notice before material model changes. Spell out which updates require a formal reassessment. And make sure vendors are required to join root-cause analysis if an AI-related safety event happens. Censinet RiskOps and Censinet AI can centralize vendor evidence, map controls, flag gaps, and trigger reassessment when vendors change.
ONC's HTI-1 Final Rule requires AI and predictive models embedded in certified health IT to disclose intended use, training data, performance, fairness and bias information, and limitations.[23][24][26] Treat those disclosures as the floor, not the ceiling. If a vendor can't meet that bar, that's a warning sign to act on before go-live.
Conclusion: 5 controls that most directly protect patients
Those controls boil down to five practical actions.
| Control | What it does |
|---|---|
| Maintain an AI inventory | Know, own, and classify every deployed tool |
| Validate high-risk use cases | Confirm performance in your population before and after go-live |
| Monitor for drift and unsafe outputs | Catch silent failures before they reach care decisions |
| Keep humans in critical decisions | Prevent over-reliance in high-stakes clinical moments |
| Build AI-specific incident response and vendor assurance into governance | Treat AI failures as patient-safety events |
ECRI ranked "Risks with AI-enabled health technologies" as the #1 health technology hazard for 2025[11][22], and the Joint Commission treats AI-related safety events as analogous to other patient safety events.[25] That framing matters. AI resilience isn't just a tech project. It's a patient-safety discipline, and it calls for the same rigor, accountability, and steady attention that healthcare organizations already apply to medication safety, device management, and infection control.
FAQs
What makes AI resilience different from AI governance?
AI governance sets the structure, policies, and accountability for managing AI across its lifecycle. It spells out ownership, risk tiers, and compliance expectations.
AI resilience is about how AI systems hold up, adjust, and recover when things go wrong in practice. Governance sets the rules; resilience helps keep AI secure, reliable, and safe under pressure.
How often should hospitals revalidate high-risk AI tools?
High-risk AI tools should be reassessed quarterly. Lower-risk tools should be reviewed at least annually.
Teams should also use continuous monitoring and revalidate when processes change, new equipment is introduced, or the model starts to drift. That way, AI tools stay accurate and safe as data and software shift over time.
What should trigger an AI shutdown or rollback?
An AI shutdown or rollback should happen when a system drops below promised benchmarks, shows signs of major clinical harm, or runs into a critical security incident.
That line needs to be clear before anything goes wrong. Teams should spell out stop criteria and rollback plans in their AI governance rules and incident response playbooks. If a model update performs worse than the previous version, that’s a red flag. The same goes for model drift that cuts accuracy over time.
Put simply: if the system is no longer meeting the bar it was supposed to meet, or if it starts putting people or data at risk, there should be a plan to pause it, roll it back, and act fast.
