PKI is how I prove that a user, device, or system should be trusted before it touches PHI. It helps me lock data in transit, confirm who is on each end of a connection, sign records and messages, and shut off access when a certificate expires or must be revoked.
If I had to boil the whole topic down, it comes to this:
- Keys encrypt data and verify signatures
- Certificates link those keys to a person, device, app, or server
- Certificate authorities and registration authorities issue certificates after identity checks
- Revocation and expiration checks help stop use of bad or old certificates
- HSMs, TPMs, and policy rules help keep private keys safe
- TLS, mTLS, S/MIME, Direct messaging, FHIR APIs, portals, telehealth, and medical devices all rely on PKI in day-to-day healthcare
- The main failure point is often poor certificate tracking, not the math behind encryption
A few points stand out fast:
- HIPAA points to identity checks, access control, transmission security, and audit controls
- One missed renewal can block portal logins, EHR links, or API traffic
- In California, an expired certificate issue delayed or lost more than 300,000 COVID-19 test results
- Large health systems may have thousands of certificates across cloud apps, devices, interfaces, and partner connections
If I’m looking at PKI for PHI, I focus on three questions first:
- Who gets trusted?
- How is that trust checked?
- Who owns renewal, revocation, and key protection?
That’s the article in plain English: PKI is less about theory and more about keeping certificates, keys, devices, people, and policy in sync so PHI stays private, unchanged, and available when care teams need it.
Core PKI concepts healthcare teams should understand
Public keys, private keys, and asymmetric cryptography
PKI relies on a linked public/private key pair [2][6]. The public key encrypts data for a single recipient, and only the matching private key can decrypt it [1][3].
That same private key also creates digital signatures. The public key then verifies those signatures to confirm authenticity and integrity [2][1]. For clinical documents, that signature also supports non-repudiation [1].
To cut the risk of theft or misuse, private keys should be stored in HSMs for servers and TPMs for devices [4].
A key pair matters only when a certificate ties it to a verified identity.
Digital certificates and trust chains
X.509 digital certificates tie a public key to a verified identity, such as a clinician, a medical device, or a server, and a trusted Certificate Authority (CA) signs that certificate [2][1].
Trust moves through a hierarchy. A root CA signs intermediate CAs, and those intermediates issue certificates to end entities like patient portals and FHIR APIs [1][6]. This setup helps contain damage. If one issuing CA is compromised, it can be revoked without taking down the whole trust system [8][6].
An RA checks identity before sending a certificate request to the CA [5][2].
Revocation, expiration, and status checks
Trust doesn't stop when a certificate is issued. Its status has to stay current. Expiration sets a time limit on how long a credential stays active, which cuts the window for cryptographic attacks.
Sometimes, though, a certificate has to be canceled before it expires. A clinician may leave a practice, a device may be retired, or credentials may be stolen. That's where revocation comes in.
Two methods handle status checks:
- Certificate Revocation Lists (CRLs) are published lists of revoked certificate serial numbers that clients download on a set schedule.
- Online Certificate Status Protocol (OCSP) checks the status of one certificate in near real time [6][7].
If a certificate is expired or revoked, EHR and portal access can fail. That's why automated renewal and status checks matter.
sbb-itb-535baee
Implementing PKI for Medical Devices: A Practical Guide
The main components of a healthcare PKI
Those trust rules rest on four working parts: the CA, RA, repository, and key controls.
Certificate authorities, registration authorities, and repositories
The Certificate Authority (CA) issues and signs digital certificates for clinicians, servers, and medical devices. In healthcare, PKI often follows a tiered setup: an offline Root CA signs intermediate CAs, and those intermediate CAs handle day-to-day certificate issuance. That split lowers risk if an issuing CA is ever compromised.
Before the CA issues any certificate, the Registration Authority (RA) handles identity vetting. It checks the claimed identity of a patient, provider, or connected device. This step also supports the HIPAA Security Rule requirement at 45 CFR §164.312(d), which requires covered entities to verify the identity of entities communicating ePHI [10].
After certificates are issued, a certificate repository - usually an LDAP- or HTTP-based directory - stores them and their metadata [3][10]. If that repository is dependable, systems can find and validate active certificates during exchange without a hitch.
Once certificates are issued and published, the next job is protecting the keys behind that trust.
Key management, HSMs, and policy controls
A CA hierarchy falls apart if private keys are exposed. Hardware Security Modules (HSMs) keep private keys inside tamper-resistant hardware and block unauthorized export of the keys that protect EHR access and medical device telemetry —a critical part of managing healthcare cyber risks [4]. The Root CA private key should stay in an offline, FIPS 140-3 validated HSM and come online only for rare key ceremonies, such as signing a new subordinate CA [10][11][9].
Key management covers the full lifecycle:
- key generation
- rotation
- backup
- destruction
Certificate renewal should be automated to avoid outages. Short certificate lifespans make manual tracking risky, and one missed renewal can block clinician access to PHI with no warning [4][11].
Policy controls spell out how certificates are issued, used, renewed, and revoked. A Certificate Policy (CP) sets the standards for who can get a certificate and under what conditions. A Certification Practice Statement (CPS) lays out the operating procedures used to meet those standards. Together, they form the governance framework that helps meet HIPAA obligations.
Where PKI governance fits into healthcare risk management
PKI governance needs to tie directly to identity and device lifecycle management. When a clinician joins, changes roles, or leaves - or when a medical device is retired or a vendor relationship ends - certificate status needs to change right away. If that link breaks, trust lingers where it shouldn't.
Third-party vendor risk management adds another layer. Business associates and third-party technology vendors often run systems that depend on a healthcare organization's PKI, which can create risk exposure that's easy to miss. Folding PKI status into a broader enterprise risk process helps keep certificate gaps in plain sight.
How PKI protects PHI in real healthcare workflows
Once the PKI setup is in place, the next part is simple: how it protects PHI during day-to-day care.
Securing EHR access, portals, APIs, and health data exchange
PKI helps lock down portal logins, EHR connections, and health data exchange. TLS server certificates encrypt the connection between a browser and a patient portal, which keeps PHI from being read while it moves across the network. That matters for any patient-facing system where private data is constantly in motion.
For higher-risk server-to-server workflows, like an EHR pulling lab results or connecting to a payer, mutual TLS (mTLS) checks both sides of the connection. In plain English, each system has to prove who it is before data moves. For FHIR apps, PKI secures server-to-EHR connections. HIEs rely on federated trust bundles to verify partner identities.
Protecting email, telehealth, and connected medical devices
S/MIME and Direct Secure Messaging use PKI to encrypt clinical email and digitally sign referrals. That means only the intended recipient can read the message, and the sender’s identity can be checked. In a clinical setting, that’s a big deal. A referral, discharge note, or lab follow-up shouldn’t end up exposed or come from someone pretending to be a trusted sender.
For telehealth, PKI protects remote sessions with strong TLS encryption and tokens tied to client certificates. This helps protect patient privacy and gives clinicians more confidence that the person on the other end is who they claim to be.
Connected medical devices - infusion pumps, imaging systems, and patient monitors - bring a different kind of problem. A private CA issues a separate certificate to each device. Those certificates support secure boot, signed firmware, and encrypted telemetry. The result is pretty direct: blocked firmware that shouldn’t be there and better protection for device data in transit.
Common PKI challenges in healthcare environments
These controls can work very well, but healthcare systems are messy. Scale, older systems, and huge numbers of certificates can turn a sound setup into an operations headache.
The biggest daily risk is certificate sprawl. Healthcare organizations often manage thousands of certificates across EHR interfaces, cloud workloads, mobile devices, and IoMT endpoints. Without one central inventory, expiration dates slip through the cracks. In California, expired digital certificates disrupted the state’s COVID-19 reporting system, causing more than 300,000 test results to be delayed or lost [12].
Older devices make this worse. Many can’t support modern automated enrollment protocols, so teams end up using manual certificate handling - or skipping it altogether. A common fix is network segmentation and gateway TLS termination. That way, the older device sits behind a controlled boundary instead of talking over an unprotected channel.
The weak spots are usually operational, not cryptographic.
| PKI Challenge | Clinical Impact | Mitigation |
|---|---|---|
| Certificate expiry | Portal outages, blocked EHR access | Automated lifecycle management (CLM) |
| Legacy IoMT devices | Insecure telemetry, no device identity | Network segmentation, gateway TLS |
| Shared workstations | Slow authentication, workflow friction | Proximity cards, virtual smart cards |
| Certificate sprawl | Missed expirations, visibility gaps | Continuous discovery scans, centralized inventory |
Choosing and governing a PKI approach for PHI security
PKI Deployment Approaches for Healthcare: A Visual Comparison
Understanding PKI concepts is one thing. Deciding how to deploy and govern it across a healthcare organization is a different job entirely. The best fit depends on your systems, your team’s bandwidth, and how much compliance pressure you’re under.
PKI deployment approaches for healthcare: a comparison
Once the trust model is clear, the next call is simple in theory but messy in practice: where should control live? Inside the organization, with a managed provider, or down at the device layer.
There’s no one-size-fits-all PKI model for healthcare. The right choice should match your systems, staff, and compliance load.
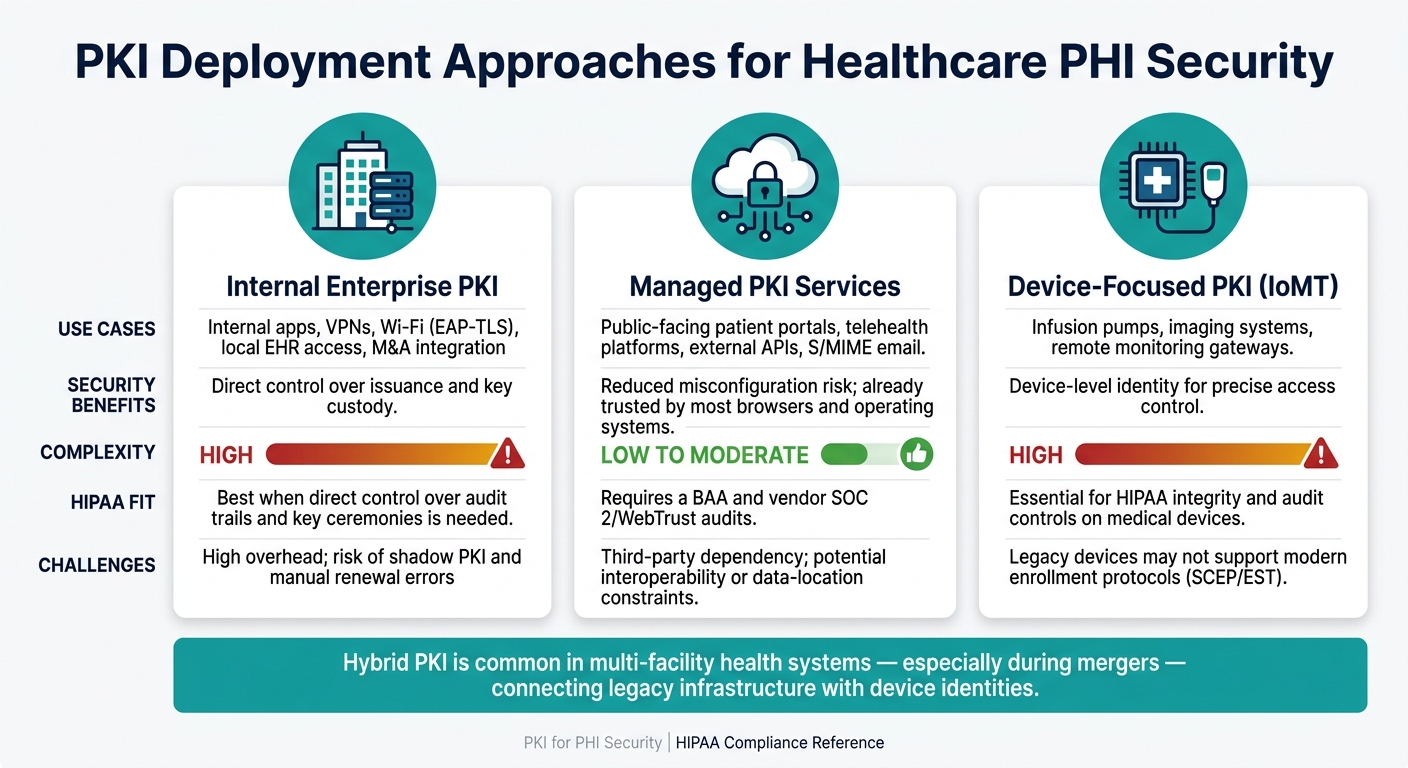
| Deployment Approach | Primary Use Cases | Security Benefits | Operational Complexity | HIPAA/Compliance Considerations | Common Challenges |
|---|---|---|---|---|---|
| Internal Enterprise PKI | Internal apps, VPNs, Wi-Fi (EAP-TLS), local EHR access, M&A integration | Direct control over issuance and key custody | High; requires dedicated crypto expertise and root key ceremonies | Best when you need direct control over audit trails and key ceremonies | High overhead; risk of shadow PKI and manual renewal errors |
| Managed PKI Services | Public-facing patient portals, telehealth platforms, external APIs, S/MIME email | Reduced misconfiguration risk; already trusted by most browsers and operating systems | Low to moderate; vendor manages CA operations and uptime | Requires a BAA and vendor SOC 2/WebTrust audits | Third-party dependency; potential interoperability or data-location constraints |
| Device-Focused PKI (IoMT) | Infusion pumps, imaging systems, remote monitoring gateways | Provides device-level identity for precise access control | High; must support SCEP and EST plus maintenance windows | Essential for HIPAA integrity and audit controls on medical devices | Legacy devices may not support modern enrollment protocols |
Hybrid PKI is common in multi-facility health systems, especially during mergers, because it helps connect legacy infrastructure with device identities.
Implementation priorities for U.S. healthcare organizations
After you pick a model, the next step is putting controls in place so the whole thing doesn’t turn into a certificate fire drill six months later.
Under the current HIPAA Security Rule, encryption is a required standard.
Deployment only holds up when certificate inventory, ownership, and renewal are handled as part of PHI security. A practical starting sequence looks like this: map your PHI data flows first. Every database, API, and device that touches PHI needs to be accounted for before you can tell where certificates are needed.
From there, use discovery data to assign owners, renewal dates, and alerting. Then set clear ownership across security, IT, compliance, clinical engineering, and third-party risk management. If no one owns a certificate, it usually means everyone assumes someone else does.
Once ownership is clear, standardize your protocols. Set TLS 1.2 or 1.3 as the baseline for data in transit. Disable obsolete versions such as SSL and TLS 1.0/1.1, along with weak hashing algorithms like SHA-1. For high-risk service-to-service workflows - EHR integrations, e-prescribing, and FHIR APIs - use mutual TLS (mTLS) so both endpoints are authenticated.
Finally, automate certificate lifecycle management with protocols like ACME, SCEP, or EST. At scale, manual renewal is where good plans start to crack.
Conclusion: Key PKI basics for healthcare leaders
The practical test of PKI isn’t the cryptography alone. It’s whether certificates, keys, and policies stay in sync over time.
PKI makes trusted identity, encryption, and integrity possible across healthcare systems. The bigger risk comes from weak governance: expired certificates, poor key control, and unmanaged third parties.
FAQs
Why does PKI matter for HIPAA compliance?
PKI matters for HIPAA compliance because it helps enforce access control, transmission security, data integrity, and auditability for PHI.
With digital certificates, PKI can verify users, devices, and applications before they get access. That helps limit sensitive data to authorized parties and supports encryption for PHI both at rest and in transit.
What happens when a certificate expires?
When a digital certificate expires, an organization loses its ability to verify the identity of a device, user, or application. That can lead to service outages and open the door to security gaps.
In settings that handle PHI, expired certificates can disrupt secure data exchange and create compliance issues. The fix is pretty simple in theory: track certificates across their lifecycle and renew them before they expire.
How should healthcare teams manage certificate renewals?
Healthcare teams should put automation at the center of the certificate lifecycle, from request and approval to issuance, deployment, and renewal. Manual work takes time, invites mistakes, and makes expired certificates and security gaps more likely.
It also helps to watch renewal windows early, not at the last minute. Teams can automate reissuance before clinical cutoffs and check that key usage flags and subject alternative names still match what each system needs.
