If a connected medical device is hit, this can become a patient safety issue in minutes - not just an IT issue.
I’d sum up the article like this: U.S. healthcare teams need passive, low-latency monitoring for IoMT devices because many devices can’t run agents, can’t be patched fast, and can’t be scanned during care. The article shows what to watch, which threat behaviors matter most, how to respond without harming care, and how to keep the program in check from purchase through retirement.
Here’s the short version:
- Why this matters: IoMT devices sit close to care delivery, so outages, bad telemetry, and device lockouts can affect treatment.
- Why IoMT is different: Many devices use legacy or vendor-specific systems, support limited software changes, and rely on passive visibility instead of endpoint tools.
- What to detect first: firmware or telemetry tampering, ransomware on device platforms, lateral movement, odd outbound connections, and config drift.
- What data to use: network flows, protocol metadata, DNS, DHCP, VLAN context, firewall logs, auth logs, and cloud logs.
- What works best: behavioral and protocol-aware detection, backed by baselines by device type.
- How to respond: validate alerts first, then match containment to clinical risk, with biomed or clinical sign-off before taking a device off the network.
- How to govern it: test rules before rollout, review alert quality each month, run tabletop drills each quarter, and track device risk across procurement, onboarding, use, and retirement.
A few numbers make the risk clear: healthcare breach costs now average $11.2 million, ransomware aimed at hospital IoT is up 68% year over year in 2026, and a 500-bed hospital may have 10,000 to 15,000 connected devices to monitor.
| Area | What the article says |
|---|---|
| Main goal | Spot threats fast enough to reduce care disruption, PHI loss, and device downtime |
| Monitoring style | Passive, stream-first, low-latency |
| Top telemetry | Flows, protocol data, DNS/DHCP, VLAN, firewall, auth, cloud |
| Top response rule | Don’t remove a device from service without clinical or biomed approval |
| Program control | Monthly alert review, annual re-checks, lifecycle tracking, vendor access rules |
If you want one takeaway, it’s this: IoMT threat detection has to be fast, passive, and tied to clinical decision-making - not just SOC workflows.
IoMT Threat Landscape and Detection Requirements
Ransomware aimed at hospital IoT jumped 68% year over year in 2026, and the average healthcare breach now costs $11.2 million [2]. At the same time, a 500-bed hospital may have 10,000 to 15,000 connected devices in use. That’s a lot to watch, and it changes the job. Instead of trying to stop every possible threat at the edge, security teams need to spot the few behaviors most likely to interrupt care - and spot them fast.
High-Risk Attack Surfaces in Connected Medical Devices
One major risk is firmware supply-chain compromise. In plain terms, attackers slip malicious code into device updates before those updates ever reach the hospital [2]. Another weak spot is poor network segmentation. If a blood-gas analyzer is compromised on a flat VLAN, an attacker can move from that device to EHR servers in minutes [2]. Vendor remote access also creates risk, especially when attackers use AI-generated phishing and deepfakes to steal service credentials [2].
Those entry points may look different on paper, but they tend to lead to the same handful of behaviors that matter most in day-to-day hospital defense.
Threat Behaviors Security Teams Should Detect First
Not every alert deserves the same level of urgency. Some behaviors are far more likely to affect patient care, lock up devices, or expose PHI. The table below shows which ones should move to the front of the line:
| Detection Priority | Threat Behavior | Clinical/Operational Risk |
|---|---|---|
| High | Firmware or telemetry manipulation | Patient safety (incorrect dosage/data) |
| High | Ransomware on RTOS-based devices | Device lockout; total care disruption |
| Medium | Lateral movement | PHI exfiltration; EHR compromise |
| Medium | Unusual outbound IP connections | Data exfiltration; C2 communication |
| Low | Unauthorized configuration drift | Compliance failure; security gap creation |
The danger here isn’t abstract. In January 2026, attackers compromised 1,400 infusion pumps across three campuses and altered dosage telemetry. The problem went undetected for 11 days [2].
Minimum Detection Capabilities for Healthcare Operations
Detection has to make up for patching gaps. 53% of connected medical devices have at least one known critical vulnerability left unpatched, and manufacturers fix only about 1 in 50 known vulnerabilities [3]. If patching can’t keep pace, monitoring has to.
That starts with continuous, passive asset visibility rather than quarterly scans. Security teams need a live view of what’s on the network, which firmware version each device is running, and how those devices communicate [2]. Without that, it’s hard to tell normal device behavior from the start of an attack.
The baseline also needs support for segmented networks and microsegmentation policies that separate device classes such as imaging, infusion, and telemetry [2][3]. Active scanning, on the other hand, is mostly off the table in clinical settings.
"Running an active vulnerability scan on an infusion pump mid-infusion risks disrupting the treatment... Security controls for IoMT have to work around the clinical workflow, not the other way around." - Asimily [3]
sbb-itb-535baee
Detection Architecture and Telemetry for IoMT Monitoring
IoMT Threat Detection Methods: Speed, Accuracy & Clinical Impact
Core Components of an IoMT Detection Stack
Once you’ve defined the highest-risk behaviors, the next job is building a stack that can spot them without getting in the way of patient care. In IoMT, that matters a lot. You can’t just poke at devices and hope nothing breaks.
A solid IoMT detection stack needs to do three things well: collect passive telemetry, analyze it in real time, and trigger a response without touching the device itself. That’s why a stream-first architecture works well here. It handles continuous data with low latency instead of waiting for batch jobs to run [5].
To avoid putting pressure on devices with limited resources, teams can train models offline and then deploy lightweight edge classifiers at the edge [4]. That approach keeps analysis close to the action while leaving the device alone.
At the analytic layer, hybrid models can pick up both communication patterns and time-based behavior shifts [6][7]. Many setups also include closed-loop retraining and policy updates, so access rules can change as behavior drifts over time. And when alerts come with explainable outputs, clinical teams have a much better shot at understanding why something was flagged [4].
That stack only works, though, if it pulls in the right signals.
Telemetry Sources That Produce Actionable Alerts
The telemetry that tends to matter most for IoMT monitoring comes from network flows, protocol metadata, DNS and DHCP logs, VLAN context, firewall events, authentication logs, and cloud service logs. Put together, these sources show which devices are talking, how often they do it, and where that traffic is going.
When traffic is encrypted, payload inspection won’t help much. In those cases, security teams should lean on packet timing, flow volume, connection frequency, and destination reputation instead [6].
"The communication patterns between devices can fluctuate based on patient conditions, device configurations, and environmental factors, making it difficult for traditional IDSs to distinguish between benign and malicious activity." - Jamshed Ali Shaikh, Chongqing University [7]
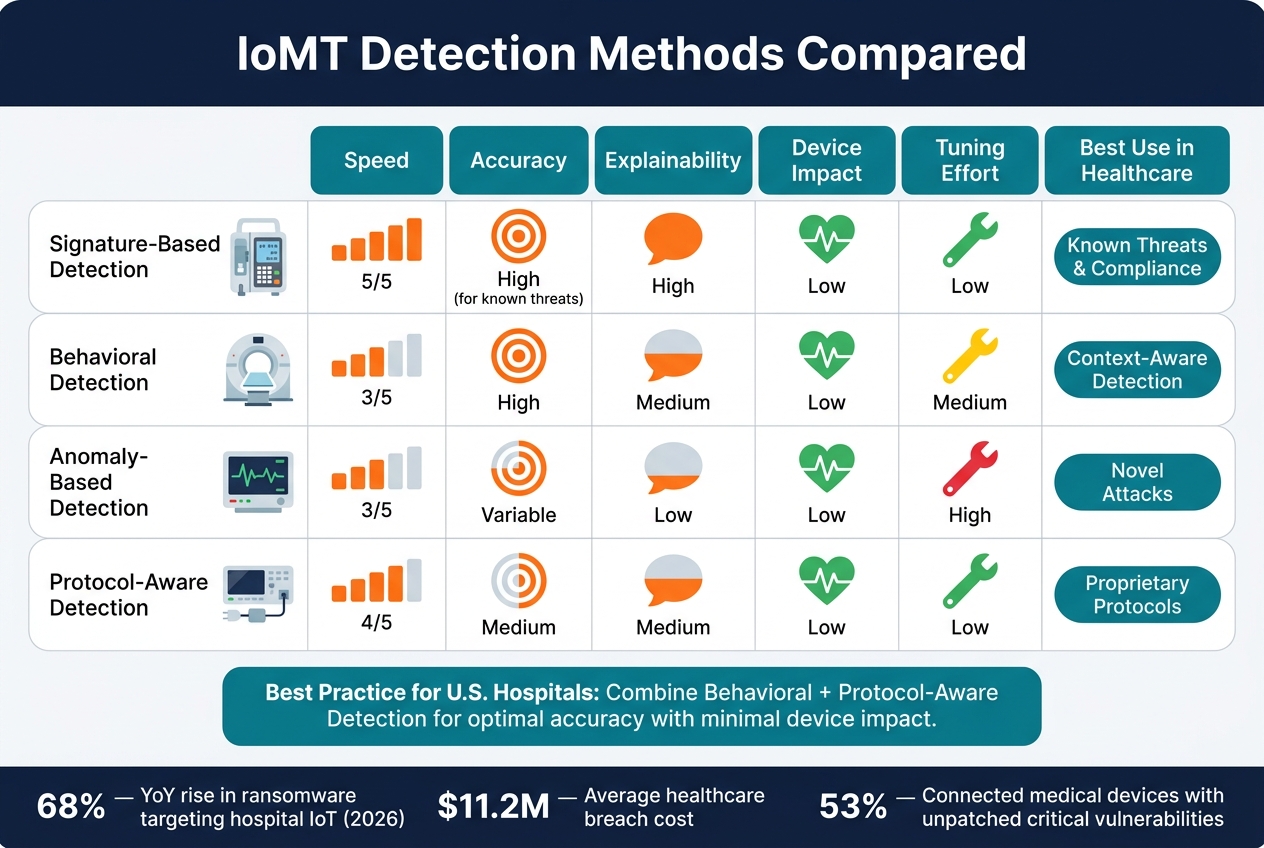
Detection Methods Compared: Speed, Accuracy, and Device Impact
The right detection method has to do more than flag odd behavior. It has to protect patients. That’s the standard. And because different methods fit different device types, the tradeoffs matter.
Each method gives up something for something else. Some are fast but narrow. Others catch more unusual behavior but take more tuning.
| Detection Method | Speed | Accuracy | Explainability | Device Impact | Tuning Effort | Best Use in Healthcare |
|---|---|---|---|---|---|---|
| Signature-based | Very High | High for known threats | High | Low | Low | Strong for compliance and known threats |
| Behavioral | Medium | High | Medium | Low (passive) | Medium | Strong for context-aware detection |
| Anomaly-based | Medium | Variable | Low | Low | High | Useful for novel attacks, but can create false positives |
| Protocol-aware | High | Medium | Medium | Low | Low | Important for proprietary medical protocols |
In most U.S. hospital settings, behavioral plus protocol-aware detection tends to give the best mix of accuracy and low device impact. Behavioral and protocol-aware methods usually fit healthcare best, while anomaly detection tends to work better after baselines have had time to settle.
Implementation and Real-Time Response Workflows
How to Deploy Detection Without Disrupting Care Delivery
After you define telemetry and detection methods, roll out deployment in phases so care delivery stays intact. Start with the basics: validate your inventory and continuous monitoring capabilities, place passive sensors at key VLAN boundaries, and baseline behavior by device type. That last step matters more than it may seem, because a bad deployment choice can interfere with treatment.
A pilot in one clinical segment is the safest place to start. It gives the team room to tune thresholds and spot coordination issues between clinical engineering, biomed, and the security operations center (SOC). Those groups need to move in sync before any alert turns into a live response.
Once rollout is in place, the main goal changes. At that point, it’s no longer just about visibility. It’s about responding fast without putting patients at risk.
Triage, Containment, and Escalation for IoMT Incidents
When an alert fires, the first step is validation. Security teams should correlate network behavior, model-specific vulnerabilities, and indicators of compromise (IOCs) [1].
After that, the response should fit the device’s clinical role and the urgency of the risk. Manual approval should be required before isolating a device or removing it from service. That keeps clinical risk, not just security severity, at the center of each decision. High-confidence alerts tied to patient-care devices should go to clinical engineering and biomed. If remediation depends on the vendor, escalate to the vendor at the same time.
Response Options Compared by Urgency and Clinical Risk
Response actions should match both urgency and patient risk. The table below compares the main options by impact and approval level.
| Response Option | Urgency | Operational Impact | Patient Safety Risk | Approval Level |
|---|---|---|---|---|
| Monitoring Only | Low | None | Low | None (Standard SOC) |
| Blocking Specific Traffic | Medium | Low to Medium | Low | Security Team |
| Isolating a VLAN | High | Medium | Moderate | Security + IT Admin |
| Network Removal | Critical | High | High | Clinical/Biomed Lead |
| Vendor Remediation | Low to Medium | Variable | Low | Vendor + Biomed |
The approval column is the one to watch most closely. A device should not be removed from the network without sign-off from clinical or biomed teams. That step needs to be built into playbooks before an incident puts everyone on the spot.
Governance, Validation, and Lifecycle Operations
Risk Ownership, Validation, and Control Validation
Once detection is live, governance is what keeps alerts accurate, approved, and safe for clinical use.
A federated governance model works best when an enterprise risk committee leads it. The CISO should own the detection program. IT should handle network visibility and segmentation. Biomed should manage device inventory and safety checks. Compliance should cover HIPAA and audit reporting. Procurement also has a job here: bake security requirements, data-sharing terms, and detection integration needs into RFPs and contracts before a device goes live.
Validation also can't be treated like a one-and-done task. Before you turn on new detection rules or behavior models, test them against representative devices in a lab or test network when possible. In production, phase changes in slowly. Keep new rules in monitor-only mode until the team confirms they work as expected. If a change affects a live clinical device, biomed needs to sign off on it, and there needs to be a rollback plan in place. Re-validate at least once a year, or any time major firmware or platform updates happen.
To keep the program tight over time, run monthly alert quality reviews. Security analysts and biomed should review alerts together, sort out false positives, allowlist known vendor update servers, and point out missing detections. A few metrics matter most here:
- Mean time to detect (MTTD)
- False-positive rate by device class
- Percentage of critical devices covered by high-confidence detections
Quarterly tabletop exercises should bring together security, biomed, IT, and clinical leadership. Walk through realistic scenarios, like ransomware on an imaging segment or unauthorized remote access to infusion pumps. That kind of practice exposes gaps in runbooks and escalation paths before a live incident forces the issue.
Device Lifecycle Governance and Third-Party Coordination
Those same validation controls need to carry through procurement, onboarding, operations, and retirement.
Security checkpoints should be built into each stage of the device lifecycle, not added after deployment. At procurement, require SBOMs, MDS2 forms, vulnerability disclosure commitments, and patch SLAs as purchase conditions. At onboarding, log the model, firmware, IP/MAC, clinical owner, and network segment in the CMDB before go-live. Then use the first 30 days to baseline normal behavior before turning on high-sensitivity alerts.
During operations, patches and firmware updates need to be coordinated with clinical leadership and change control boards so scheduled procedures aren't disrupted. If patches aren't available, document time-bound risk exceptions, put compensating controls in place, and review those exceptions every quarter. That may include stricter segmentation, virtual patching through next-generation firewalls, and closer monitoring. The goal is simple: keep detection coverage in place even when patching can't happen.
At decommissioning, revoke access, disable vendor connections, confirm data sanitization, and remove the device from both monitoring and inventory.
Third-party access should follow the exact same governance rules because vendor connections often carry the highest operational risk. Contracts should spell out allowed remote support protocols, multi-factor authentication requirements, logging expectations, and notification steps for suspicious activity. Censinet RiskOps™ can centralize third-party risk assessments, vendor evidence, benchmarking, and collaborative remediation across suppliers and internal security teams.
Conclusion: What an Effective IoMT Detection Program Must Deliver
An effective IoMT detection program delivers continuous visibility, clinically safe response, validated baselines, and governance that brings together cybersecurity, clinical operations, and vendor risk.
FAQs
Why is passive monitoring so important for IoMT devices?
Passive monitoring matters for IoMT devices because it lets healthcare teams find, classify, and track assets without actively probing them. That’s a big deal in clinical settings, where even small disruptions can affect sensitive equipment or interrupt care.
Instead of touching the device, passive monitoring watches network traffic and protocols like DICOM and HL7. This gives teams a clearer view of devices that might otherwise stay hidden. It also helps them build behavior baselines, spot unusual activity, and respond to threats in real time, all without getting in the way of patient care.
How can hospitals respond to IoMT threats without disrupting care?
Hospitals can cut IoMT risk without disrupting care by using passive, non-intrusive security methods. Passive network discovery watches device behavior and spots threats in real time, all without touching sensitive medical equipment or interrupting clinical work.
Adding clinical context to anomaly detection helps cut false alarms. And with microsegmentation and Zero Trust policies, teams can isolate suspicious devices or traffic while keeping critical patient workflows running.
What should healthcare teams baseline first for real-time detection?
First, build a complete and accurate asset inventory. If you can’t see the full IoMT environment, you can’t detect threats in real time. It’s that simple.
Next, sort and rank devices by risk. Look at:
- Clinical impact
- Technical vulnerabilities
- Exposure
Once that groundwork is done, teams can use passive network visibility to set behavioral baselines and spot anomalies in real time.
