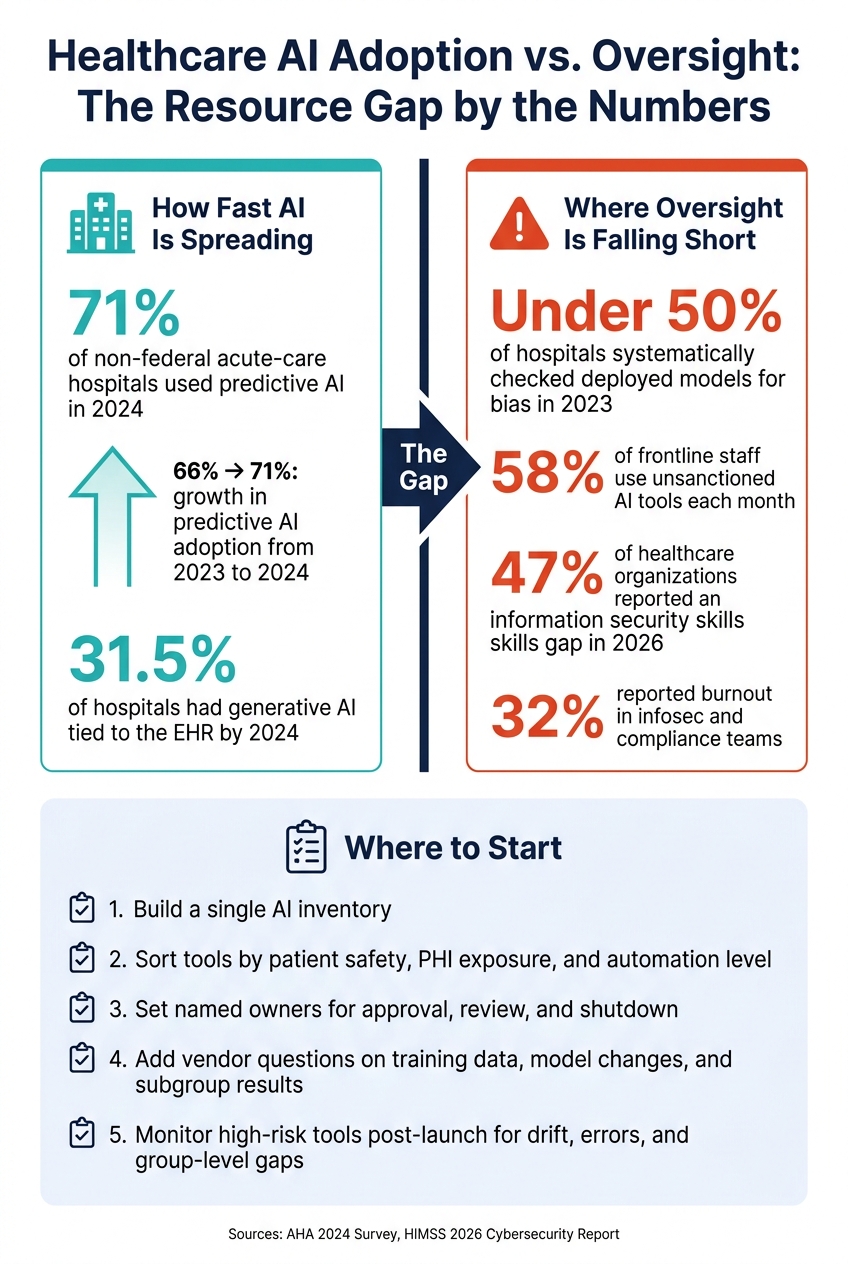
Hospitals are putting AI into care and workflow faster than they can review it. In 2024, 71% of non-federal acute-care hospitals used predictive AI, and 31.5% already had generative AI tied to the EHR. But many teams still lack a full AI list, clear owners, vendor detail, and post-launch checks.
If I had to sum up the problem in plain English, it’s this:
- AI adoption is outpacing oversight
- Vendor tools often arrive inside systems hospitals already use
- Many hospitals still don’t test enough for bias or accuracy after launch
- Staff, budget, and time limits leave reviews stuck in email and spreadsheets
- Shadow AI use by frontline staff adds more risk
- The fix is to start with high-risk use cases, assign owners, and use one repeatable review process
A few numbers make the gap hard to ignore:
- 66% to 71%: growth in predictive AI adoption from 2023 to 2024
- 31.5%: hospitals using generative AI in the EHR by 2024
- 58%: frontline staff using unsanctioned AI tools each month
- 47%: healthcare groups reporting an information security skills gap in 2026
- Under 50%: hospitals that systematically checked deployed models for bias in 2023
What should hospitals do first?
- Build a single AI inventory
- Sort tools by patient safety, PHI exposure, and level of automation
- Set named owners for approval, review, and shutdown
- Add vendor questions on training data, model changes, and subgroup results
- Watch high-risk tools after launch for drift, errors, overrides, and group-level gaps
This is not just a policy issue. It’s a day-to-day risk issue that affects patient care, compliance, and staff workload.
In short: before hospitals expand AI use, they need a lean system for inventory, review, vendor checks, and post-launch monitoring.
Healthcare AI Adoption vs. Oversight: The Resource Gap by the Numbers
Where the Resource Gap Appears Across the AI Lifecycle
Staffing, Governance, and Time Constraints
The staffing problem isn't just about headcount. It's about missing the people who can connect clinical, data, security, and compliance risk in one place.
In many hospitals, clinical, IT, security, and compliance teams review AI in silos. That sounds manageable on paper, but in practice it means no one owns end-to-end risk before deployment. The first cracks usually show up during acquisition and validation.[2][4][5]
The pressure is even worse because the same teams asked to oversee AI are already stretched thin. In 2026, 47% of healthcare organizations reported an information security skills gap, and 32% cited burnout in infosec and compliance teams.[11] Those are often the exact people expected to review AI tools, flag problems, and keep oversight moving.
Many hospitals do have governance committees. The issue is that some exist more as policy groups than working decision bodies. They may meet rarely, lack the power to stop a deployment, or spend most of their time on high-level planning instead of structured risk review. What hospitals need is much more direct:
- Named risk owners
- Clear decision rights
- Escalation paths
- Written records on patient impact, error types, equity risks, and override rules
When that structure is missing, teams usually fall back on manual tracking. And once AI oversight lives in side notes, inboxes, and one-off spreadsheets, things can slip fast.
Tooling and Budget Gaps
Without AI-specific tooling, risk work often gets pushed into spreadsheets, shared drives, and email. That might work for a while, but it goes stale fast. One version gets updated, another file doesn't, and suddenly the monitoring data no longer lines up with the model that's live.[4][5]
That's not just messy. It makes review harder at the exact moment teams need clean records.
Budget gaps make the problem worse. Limited funding restricts hiring and continuous monitoring, especially in community and rural hospitals that already run with small IT teams and aging infrastructure.[8][10][11] In rural settings, staff often wear multiple hats. A clinician may also act as the informal IT lead, which makes steady AI oversight hard to keep up, even when the tool is already in use.[10]
Vendor and Supply Chain Visibility Limits
AI often shows up bundled inside an EHR module or imaging platform. When that happens, hospitals may have very little visibility into how the model was built, what data trained it, or how it might behave after an update. Vendors often share limited detail about training data, updates, benchmarks, or bias testing.[2][3][4]
The contract side has a similar problem. Many agreements don't require vendors to say when a model has been retrained or when its behavior changes in a major way. That leaves hospitals unable to verify retraining, compare versions, or trace shifts in performance after deployment.[3][4][7]
That's where weak oversight turns into avoidable risk. The gaps don't stay in one step of the process, either. They spread across the full lifecycle, from inventory and vendor review to validation, monitoring, and retirement.
sbb-itb-535baee
Common Failure Patterns Caused by the Resource Gap
The resource gap takes a governance problem and turns it into day-to-day failure across operations, compliance, and patient safety. These outcomes aren't random. They tend to show up the same way, again and again, when AI programs don't have enough people, time, or process behind them.
Limited Oversight After Deployment
The most common breakdown is simple: the model goes live, and then no one watches it. A model might pass validation before launch and still slip in production if nobody tracks drift, overrides, alert volume, or subgroup performance.
The FDA and related guidance have acknowledged dataset drift and unintended bias as post-deployment risks that need active controls.[13][15][17] But many healthcare organizations still handle AI validation like a one-and-done checkpoint instead of a continuing duty.
Here’s what that gap looks like in practice:
| Pre-Deployment Checks Only | Continuous Monitoring Program | |
|---|---|---|
| Common failure modes | Undetected drift, silent bias, vendor update surprises | Caught early via threshold alerts, subgroup analysis, and scheduled performance reviews |
| Resulting risk exposure | High - degraded model operates undetected | Managed - issues are escalated before patient or operational harm occurs |
The same staffing and process shortfalls also weaken vendor review before deployment.
Weak Third-Party AI Due Diligence and Data Controls
Standard vendor review often misses AI risk. A normal security questionnaire may cover access controls and data handling, but it usually doesn't ask how the model was trained, what subgroup performance data exists, or what happens when the vendor retrains the model after deployment.
The weak spot shows up even more in contracts. Agreements often leave out update notification requirements, audit rights, or clear incident reporting timelines. That means a hospital may buy the tool, hook it into care or workflow, and still lack the terms needed to manage model change later.
| Stage | Typical Current Practice | AI-Appropriate Practice |
|---|---|---|
| Due diligence | Security questionnaire, data handling review | AI-specific questionnaire: training data, validation evidence, known failure modes, subgroup performance, bias testing |
| Contracting | Data processing agreement, liability terms | Update notification requirements, audit rights, incident reporting timelines, data use restrictions, adverse event responsibility |
| Onboarding | Access provisioning, training | Confirm logging, PHI handling, human escalation pathways, access control review |
| Ongoing monitoring | Annual renewal review | Drift tracking, vendor change logs, override behavior, performance against agreed thresholds |
Even when the contract looks complete on paper, unclear ownership can still leave the risk sitting out in the open.
Unclear Accountability, Safety, and Equity Oversight
When ownership is fuzzy, decisions slow down. Clinical, IT, compliance, and security teams may each own part of the risk, but no one owns the end result. So residual risk stays unassigned. Then, when a warning sign pops up, the response drags because nobody is clearly empowered to step in.
The risk gets sharper when hospitals deploy vendor models without local validation.[12][9][16] Regulators and expert frameworks call for subgroup analysis and real-world bias checks after deployment,[12][14][18] but that work only happens if someone is assigned to do it and has the capacity to act on what they find.
A vendor model trained somewhere else can perform unevenly across local patient groups. That's why subgroup analysis and real-world bias checks aren't optional extras. They're basic safety work.
How Healthcare Organizations Can Close the Gap
These failures usually come from ad hoc governance, not from AI itself. The fix is a repeatable operating model that works even when staff and budget are tight. So the next move is pretty straightforward: standardize governance before expanding use.
Use NIST AI RMF to Build a Lean Governance Model
The NIST AI Risk Management Framework (AI RMF), published in January 2023, is built around four functions: GOVERN, MAP, MEASURE, and MANAGE.[6][7] It's designed to work across organizations with different sizes and levels of maturity, which makes it a good fit for healthcare teams that don't have a lot of spare capacity.
A lean governance model based on the AI RMF doesn't have to be big or complicated. At a minimum, it should include:
- A complete AI inventory that tracks system name, use case, owner, data inputs, PHI exposure, risk tier, approval date, validation status, monitoring owner, and review cadence
- Risk-tier each use case by patient safety impact, data sensitivity, population vulnerability, level of automation, vendor opacity, and frequency of use
- Named approval roles with real authority - clinical, privacy, security, and compliance sign-off before deployment
- Monitoring plans for high-impact systems, with defined thresholds and escalation rules
- A risk register that documents residual risk acceptance so accountability is on record
This doesn't mean building a brand-new committee from scratch. In many healthcare organizations, existing groups - privacy committees, security councils, and clinical informatics boards - can take on the AI RMF's GOVERN function with a clear charter update and defined decision rights.
Once ownership is clear, the job becomes much easier: make sure every AI use case goes through the same assessment and monitoring process.
Standardize Assessments, Vendor Reviews, and Monitoring
Ad hoc reviews are where governance starts to slip. A short, consistent intake workflow gives every AI use case the same path to approval.
A practical intake process should capture intended use, affected populations, data sources, PHI involvement, and whether the system makes or supports decisions that affect care. That feeds a standard risk questionnaire covering privacy, security, fairness, clinical validity, explainability, and human oversight. From there, teams can assign a risk score and route the issue into enterprise risk, compliance, and HIPAA-related processes when needed.
For third-party AI risk, the same idea applies. A concise vendor checklist should cover items that standard security questionnaires often miss:
| Checklist Area | What to Ask |
|---|---|
| Training data transparency | Sources, representativeness, PHI handling |
| Validation evidence | Clinical studies, performance metrics, known failure modes |
| Intended-use limitations | Where the model should and should not be used |
| Model update protocol | Change notification timelines, re-validation procedures |
| Security, privacy, and BAA status | Encryption, access controls, HIPAA alignment |
| Subgroup performance | Equity metrics, bias testing results, remediation plans |
| Ongoing reporting obligations | Incident reporting, performance dashboards, post-deployment review support |
After intake and contracting, monitoring closes the loop. Set the review cadence by risk tier: monthly for high-risk clinical models and quarterly for lower-risk operational tools. Track a small set of indicators - performance drift, error trends, subgroup disparities, override rates, and major vendor changes - and set thresholds ahead of time so escalation is automatic, not discretionary.[7][2][4]
Use Automation and Flexible Operating Models
Even solid workflows can fall apart when teams have to run everything by hand. Automation cuts manual follow-up, duplicate entry, and coordination overhead, which helps small teams oversee more AI assets with less drift.
Censinet RiskOps™ centralizes assessments and the risk register, Censinet AI™ speeds third-party reviews, and Censinet One™ and managed services flex review capacity as demand changes.
Prioritization and Conclusion: Reducing the Highest AI Risks First
Limited staff and budgets mean one thing: triage comes first. Put the highest-risk AI systems under real oversight before spending time on lower-stakes tools.
Triage AI Use Cases by Impact and Monitoring Need
A practical place to start is sorting AI systems into four impact tiers based on clinical effect, patient safety, operational dependency, and regulatory exposure. NIST AI RMF says safety risks that could lead to serious injury or death should get the most urgent attention and the deepest risk management process.[6]
A sepsis prediction model in the ICU is not the same governance issue as an HR scheduling tool. They shouldn't go through the same level of review.
| Impact Tier | Assessment Depth | Monitoring Frequency |
|---|---|---|
| Critical (e.g., sepsis alerts, stroke routing AI, autonomous diagnostic tools) | Full clinical, technical, and ethics review; FMEA; bias analysis; local data validation; PHI, cyber, and regulatory review | Continuous or near-real-time monitoring |
| High (e.g., readmission risk scores, chronic disease prediction models) | Full review; bias testing; vendor validation evidence; security and privacy audit | Weekly to monthly monitoring |
| Medium (e.g., nurse staffing and scheduling models) | Standard risk questionnaire; fairness and quality review; vendor checklist | Monthly to quarterly checks |
| Low (e.g., back-office automation) | Basic intake and privacy review | Change-based review only |
Build an Incremental Roadmap Based on Maturity and Benchmarks
Once the tiers are in place, the next step is sequencing the work.
In days 1–30, assign AI oversight to an existing committee or set up a lean governance group with clear decision rights. In days 31–90, build an inventory of AI systems, triage critical and high-risk use cases, and begin baseline monitoring. In days 91–180, standardize assessments and vendor reviews, then benchmark maturity across GOVERN, MAP, MEASURE, and MANAGE.[2][6][1]
The maturity assessment should help rank remediation work by risk reduction, not by what's easiest to fix.
FAQs
How do we find AI already in use?
Look past standard IT procurement reviews. They often miss vendor-embedded AI that shows up later through software updates.
Instead, build a centralized, enterprise-wide AI inventory that stays current, not a static spreadsheet.
Track details like:
- System names
- Clinical and technical owners
- Use cases
- Data types
- Integration points
- Departmental dependencies
- Vendor software updates that may add new AI features
That way, you’re not just logging what was bought. You’re keeping tabs on what’s actually in use across the enterprise, including AI tools that can slip in quietly over time.
Which AI tools should we review first?
When time and staff are tight, review AI tools by risk first. Put the biggest focus on tools with the most clinical and operational impact. That usually comes down to three things: clinical impact, data sensitivity, and how deeply the tool connects to the EHR.
Start with high-risk tools. This includes direct clinical decision support, ambient documentation, and tools with read-write EHR access. Lower-risk tools, like administrative scheduling or transcription, can move through a lighter review process.
What should we require from AI vendors?
This calls for more than standard IT procurement.
Ask vendors for clear documentation on:
- system architecture
- validation protocols
- data privacy procedures
- a CHAI Applied Model Card that covers training data provenance, subgroup performance, and known failure modes
Contracts should also include AI-specific protections. That means no use of patient data for training without consent, the right to suspend or roll back tools if performance drops, 24-hour breach notification, and notice of material algorithm changes that affect safety, performance, or intended use.
