If your API gateway is weak, PHI is easier to reach. In healthcare, that can mean breach costs above $10 million and direct exposure through patient apps, EHR links, payer connections, and device APIs.
If I had to boil this article down to the main point, it would be this: I need to treat the API gateway as the first security check for every request. That means I should:
- Check identity at the edge with OAuth 2.0, OIDC, SMART on FHIR, JWT checks, TLS, and mTLS
- Limit access tightly with short-lived tokens and narrow scopes like
Patient.read - Block bad requests early with schema validation, header stripping, and response filtering
- Control traffic with route-based throttling,
429responses, concurrency caps, and circuit breakers - Log every important event with user ID, IP, resource accessed, token decision, and policy version
- Split policies by trust zone for patient apps, internal systems, third-party partners, payers, and medical devices
- Keep a live API inventory so old endpoints and shadow APIs do not stay exposed
- Match gateway rules to HIPAA, HITECH, and CMS API rules, including FHIR R4 support and payer deadlines tied to January 1, 2027
A few facts stand out. Healthcare breaches cost about 2x the cross-industry average. Payers covered by CMS-0057-F must support production-ready FHIR R4 APIs by 01/01/2027. And many common API failures are simple: broken object-level access checks, weak token settings, credential stuffing, weak FHIR query validation, and forgotten internet-facing endpoints.
So when I read this piece, the takeaway is plain: a secure gateway is not just a routing layer. It is where I enforce access, traffic limits, audit logs, PHI minimization, and route separation before requests ever touch clinical systems.
The rest of the article explains how to set those rules in a healthcare setting without leaving gaps between compliance policy and live API traffic. This alignment is critical when choosing healthcare risk solutions to manage these technical controls.
Regulatory and Architecture Foundations for Secure API Gateways
How HIPAA, HITECH, and Interoperability Rules Map to Gateway Controls
HIPAA sets the rule. The gateway turns that rule into something you can enforce.
That gap matters. A policy on paper doesn't stop a bad request. Gateway configuration does. It applies each HIPAA Security Rule safeguard at the edge, before traffic ever reaches a backend system.
Each requirement lines up with a matching gateway control. Access controls become OAuth 2.0 and SMART on FHIR token checks at the gateway, so requests are screened before they hit a backend FHIR server. Transmission security means enforcing TLS 1.3 and mTLS for system-to-system exchange across organizational lines. Audit controls mean the gateway records every request, including user identity, IP address, geolocation, and the exact resource accessed. That creates an immutable trail that supports HIPAA audit needs.
The minimum necessary standard shows up in token scoping. A scheduling app should not carry a token that opens the door to lab results. Tokens should have narrow permissions, scoped to specific FHIR resources such as Patient.read, and short expiration times so the blast radius stays small if a token is stolen.
CMS-0057-F adds day-to-day requirements for impacted payers. That includes production-ready FHIR R4 APIs by January 1, 2027, plus API usage metric reporting starting January 1, 2026. Gateway policies should reflect those differences. For example, Prior Authorization may need reserved rate-limit pools, and each required API type needs its own access controls.
| HIPAA/HITECH Requirement | API Gateway Control | What It Looks Like in Practice |
|---|---|---|
| Access Control | OAuth 2.0 / SMART on FHIR | Validate JWTs and scopes at the gateway |
| Audit Controls | Centralized logging | Record user ID, IP, geolocation, and resource accessed for every call |
| Transmission Security | mTLS & TLS 1.3 | Enforce mutual authentication for system-to-system data exchange |
| Minimum Necessary | Scoped tokens | Limit token permissions to specific FHIR resources (e.g., Patient.read) |
| Availability | Rate limiting & quotas | Prevent scraping and DoS attacks to ensure service continuity |
| Integrity | Request validation | Use OpenAPI schemas to block structurally invalid or malicious requests |
Once that baseline is in place, the next move is to split gateway policy by traffic type and trust zone.
Common HDO API Architectures and Trust Boundaries
Architecture sets the trust boundary. Gateway policy puts teeth behind it.
Not all traffic should be treated the same way. Patient traffic, partner traffic, internal traffic, and device traffic each carry different risk. That means each one needs its own gateway policy.
A Zero Trust model helps here. East-west traffic between internal systems should be authenticated, authorized, and inspected just as strictly as external traffic. The same standard should apply to connections between internal clinical systems and to links with third-party apps.
In practice, HDOs usually operate across at least four trust zones. Patient-facing apps need SMART on FHIR, tight token scopes, and rate limits. Partner and payer integrations need mTLS so a compromised third party can't pretend to be a trusted system. Internal clinical systems still need Zero Trust checks, including device health and identity validation, instead of broad trust based on network location. Medical device APIs need their own rate-limit pools to protect availability. A device sending vitals can't be throttled the way a bulk export job might be.
The gateway also needs to log the token decision, tenant, timestamp, and policy version. [3]
This separation also helps block lateral movement. If a patient app gets compromised, it should not have any route into internal clinical data or device APIs. That kind of isolation doesn't happen by accident. It takes deliberate gateway policy design, not just firewall rules.
sbb-itb-535baee
Core API Gateway Security Controls HDOs Should Enforce
Authentication, Authorization, and Encryption Policies
These controls turn the trust boundaries defined above into rules the gateway can enforce. In practice, the gateway is the first line of identity enforcement. Every healthcare API request should authenticate before it gets anywhere near PHI.
At the gateway, validate OAuth 2.0/OIDC tokens and enforce SMART on FHIR scopes. Use OAuth 2.0 for authorization and OIDC for identity. For patient-facing apps, enforce SMART on FHIR launch contexts and patient-specific permissions [4][1][2]. JWT validation should happen at the gateway, which means checking the token's issuer (iss), audience (aud), expiration (exp), and scopes before the request moves downstream [1][4].
The policy should also match the traffic type. Patient-facing apps need SMART on FHIR scope enforcement. Partner and payer integrations need mTLS, so a compromised third party can't pose as a trusted system [4][2]. Internal clinical systems need Zero Trust token checks, while medical device APIs need dedicated rate-limit pools. Legacy OAuth flows such as Implicit and Resource Owner Password Credentials should be disabled in production, and certificate issuance, rotation, and revocation should be automated [4].
Input Validation, PHI Minimization, and Attack Prevention
The gateway should stop bad data at the edge instead of letting it drift into backend systems.
Validate all requests against OpenAPI schemas before they reach the backend. If a request includes malformed JSON, an unexpected parameter, or an oversized payload, the gateway should return a 400 Bad Request right away instead of passing it to a FHIR server [1][4]. Deep FHIR profile validation can still stay in the backend FHIR server.
PHI minimization matters on both the request and response side. For inbound traffic, strip unneeded headers and pass along only what the backend needs, such as Organization ID and User ID. For outbound traffic, apply response filtering and field redaction so clients don't receive more data than they should [1][2]. For highly sensitive attributes like psychiatric notes or HIV status, field-level encryption adds another layer of protection if the application layer is compromised [2].
Logs should record who accessed which resource, when, and why, without storing full patient objects or plaintext ePHI [1][4].
Rate Limiting, Resiliency, and Security Monitoring
Once identity and payload checks are in place, the gateway still needs to control traffic volume and how failures are handled.
Flat rate limits don't work well in healthcare. A better approach is tiered throttling by API type. Patient Access APIs should get per-app limits to reduce scraping risk. Provider Access APIs should get higher thresholds to support bulk operations. Prior Authorization APIs should get dedicated pools so urgent clinical requests don't get crowded out by background traffic [1]. For expensive FHIR operations like wide _include searches and $export commands, use tighter limits or send them through asynchronous queues [4]. When a client hits a rate limit, return HTTP 429 Too Many Requests with a Retry-After header so the client knows when to back off [4].
Circuit breakers, concurrency caps, and connection limits help shield the backend from cascading failures during traffic spikes [4].
After traffic is filtered and shaped, monitoring needs to spot misuse in real time. Centralized logs, normalized to the FHIR AuditEvent standard and forwarded to a SIEM with tamper-evident (WORM) storage, give security and compliance teams a strong audit trail for HIPAA-aligned review [4]. The monitoring layer should flag the abuse patterns mentioned earlier, including spikes in failed authentication attempts that match credential stuffing, patient ID enumeration, and unusual bulk record requests that may point to active data exfiltration [2].
| Control Category | Specific Gateway Policy | Healthcare Purpose |
|---|---|---|
| Rate Limiting | Per-client quotas, tiered by consumer type | Prevents scraping and resource monopolization |
| Resiliency | Circuit breakers, concurrency caps | Stops backend failures from cascading across clinical systems |
| Monitoring | Anomaly detection on query and authentication patterns | Catches ID enumeration, failed authentication spikes, and unusual bulk requests |
| Auditability | FHIR AuditEvent + WORM SIEM storage |
Supports HIPAA-aligned audit requirements |
| Error Handling | HTTP 429 with Retry-After header |
Guides client backoff without breaking clinical integrations |
Using API Gateway with FHIR API
Healthcare-Specific Deployment Patterns and Governance
Once gateway controls are in place, HDOs still need route-level rules, a clean API inventory, and close vendor oversight to keep those controls up to date.
Securing FHIR, SMART on FHIR, and Patient Access APIs
Patient, provider, and partner traffic should run through separate routes so each route can enforce its own policy.
For patient-facing apps, validate SMART on FHIR tokens at the gateway [1]. Set per-app rate limits so one third-party app can't hog system capacity [1]. Keep token scopes as narrow as possible. A scheduling app, for example, shouldn't be able to pull lab results. If a token asks for more data than the route needs, reject it [2]. FHIR requests should also be checked against OpenAPI schemas before they ever hit the FHIR server [1]. And if a patient revokes consent, data sharing with that third-party app needs to stop at once [2].
That same route separation shouldn't stop with patient apps. Internal systems, outside partners, and connected devices each need their own path and policy set.
Separating Internal, Partner, and Medical Device APIs
Use separate routes or isolated configurations for internal clinical services, outside partners and payers, and networked medical devices. Internal routes should stay on private network segments. Every internal call should still be checked for authentication and authorization based on identity, device health, and request context [2].
For partner and payer integrations, require mTLS so the client and server both verify each other [2]. On payer-to-payer links, identity-based quotas can help protect gateway capacity [1][2]. Medical device APIs need tighter isolation, including mTLS, private network limits, and strict IP allowlisting [2].
A FHIR Integration Hub behind the gateway can separate downstream apps from the details of any one EHR vendor.
Of course, segmentation falls apart fast if the API registry is stale or outside dependencies aren't being watched.
API Inventory, Third-Party Risk, and Continuous Oversight
Continuous API discovery matters because a gateway can only protect the endpoints it knows about. Keep a centralized API registry that lists every FHIR endpoint, approved scopes, consuming apps, and version dependencies [5]. Generate developer docs from OpenAPI specs so the registry matches the live implementation [1]. Under CMS-0057-F, payers must track and report API usage metrics such as requests, response times, error rates, and prior authorization turnaround times [1]. For versioned endpoints, enforce a minimum 12-month deprecation window so clinical teams and partners have time to move over [5].
Third-party integrations need the same level of review as internal endpoints. If PHI moves to a business associate through an API, that vendor's security posture becomes part of the HDO's third-party risk picture. That means vendor assessments, API security clauses, and shared incident response playbooks for every PHI-sharing integration [2].
"The gap isn't technical. The gap is organizational. It's the healthcare system that hasn't updated its threat model since it moved to the cloud." - Dr. Girirajtosh Purohit [2]
Implementation Blueprint and Conclusion
API Gateway Security Controls by Trust Zone: HDO Quick Reference
A Practical Configuration Checklist for HDO Teams
Use the controls above to turn the gateway from an idea into an edge policy you can enforce.
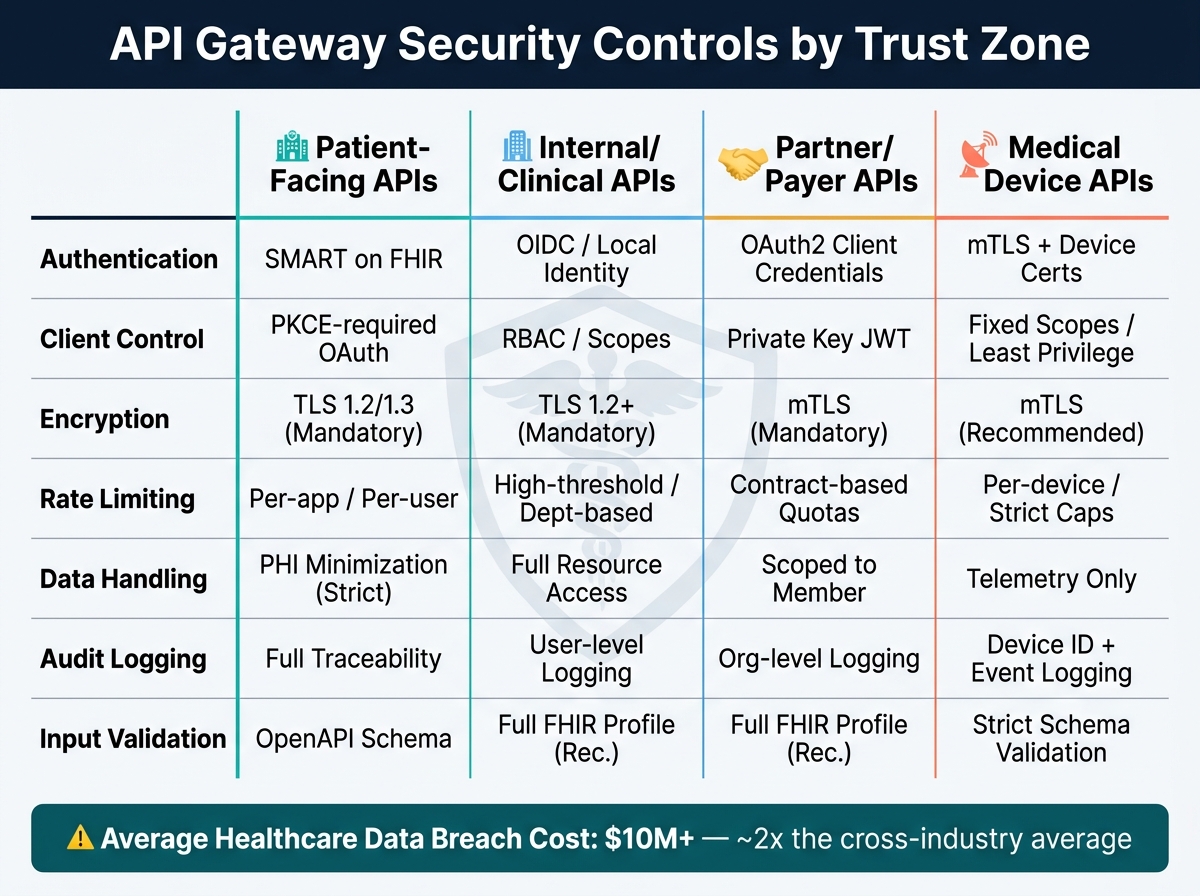
Before clinical traffic reaches the backend, the gateway should enforce TLS 1.2/1.3, mTLS to internal services, centralized authentication and token validation, scoped authorization, schema validation, PHI minimization, rate limiting, and audit logging. The right setup depends on who the API serves.
| Control | Patient-Facing APIs | Internal/Clinical APIs | Partner/Payer APIs | Medical Device APIs |
|---|---|---|---|---|
| Authentication | SMART on FHIR | OIDC / Local Identity | OAuth2 client credentials | mTLS + Device Certificates |
| Client Control | PKCE-required OAuth flow | RBAC / Scopes | Client assertion via private key JWT | Fixed Scopes / Least Privilege |
| Encryption | TLS 1.2/1.3 (Mandatory) | TLS 1.2+ (Mandatory) | mTLS (Mandatory) | mTLS (Recommended) |
| Rate Limiting | Per-app/per-user limits | High-threshold / Dept-based | Contract-based quotas | Per-device / Strict caps |
| Data Handling | PHI Minimization (Strict) | Full Resource Access | Scoped to Member | Telemetry only |
| Audit Logging | Full Traceability | User-level logging | Organization-level logging | Device ID + Event logging |
| Input Validation | OpenAPI schema validation | Full FHIR Profile (Recommended) | Full FHIR Profile (Recommended) | Strict schema validation |
A good way to start is simple: one gateway, one FHIR backend, and one introspection server. Add more only after auth and logging are stable.
Key Takeaways for Secure API Gateway Operations
Technical controls can look solid on paper and still fall apart if no one owns them day to day.
The gateway does its job only when governance stays current. With the average healthcare data breach now costing over $10 million - about double the cross-industry average [2] - this isn't just a policy exercise. It's an operating issue with direct risk tied to live traffic and PHI exposure. Censinet RiskOps™ helps HDOs keep third-party API risk reviews, vendor oversight, and security governance aligned with what is actually happening at the edge.
FAQs
How do I prioritize API gateway controls first?
Start with a centralized security layer for token validation, authentication, and authorization. Set up the gateway to validate bearer tokens, verify scopes, and enforce least-privilege access so only approved requests reach backend systems.
Next, add request validation, rate limiting, and throttling. After that, put logging, observability, and continuous monitoring in place. This layered approach gives healthcare organizations a secure, manageable, and compliant foundation.
What should I log without exposing PHI?
Log request metadata like timestamps, tenant, actor identity, route, resource type, action, status, latency, cache status, and policy decisions.
Do not log PHI, full request or response payloads, or sensitive identifiers like medical record numbers or Social Security numbers.
How often should I update my API inventory?
Review and update your API inventory on a regular schedule. A good rule of thumb is every 6 to 12 months, and sooner when security-related changes happen.
That routine helps you maintain security, compatibility, and solid risk management.
