Old vendor reviews don’t work well for AI. In healthcare, a vendor can change a model after approval, use new data, add outside AI services, or shift how PHI moves through the system - without much warning. That matters because by late 2024, 61% of healthcare groups were using third-party vendors for generative AI, and 86% of health systems were already using AI in clinical or business workflows.
If I had to boil the article down, it’s this:
- Point-in-time reviews go stale fast when models are retrained or features change.
- Basic security checks miss AI risk like prompt attacks, PHI in prompts and outputs, and weak explainability.
- Hidden fourth parties - like model providers, APIs, and labeling firms - can add risk that never shows up in a standard vendor file.
- Contracts and BAAs need AI terms, including limits on PHI use for model training and notice before model or subprocessor changes.
- Monitoring can’t stop after onboarding. I need version data, drift signals, error trends, override rates, and AI incident logs.
A few areas stand out most: model lifecycle controls, HIPAA and secondary data use, and patient safety when AI shapes clinical decisions. The article’s main point is simple: if I review AI vendors the same way I review fixed software, I can miss changes that affect privacy, care, and revenue.
To fix that, I’d treat AI use as a review trigger from intake through contract terms and post-signature monitoring.
Is AI in Your Vendor's Software Already a Healthcare Risk? HITRUST's Jason Kor on New TPRM Issues
Where Traditional TPRM Falls Short When Vendors Use AI
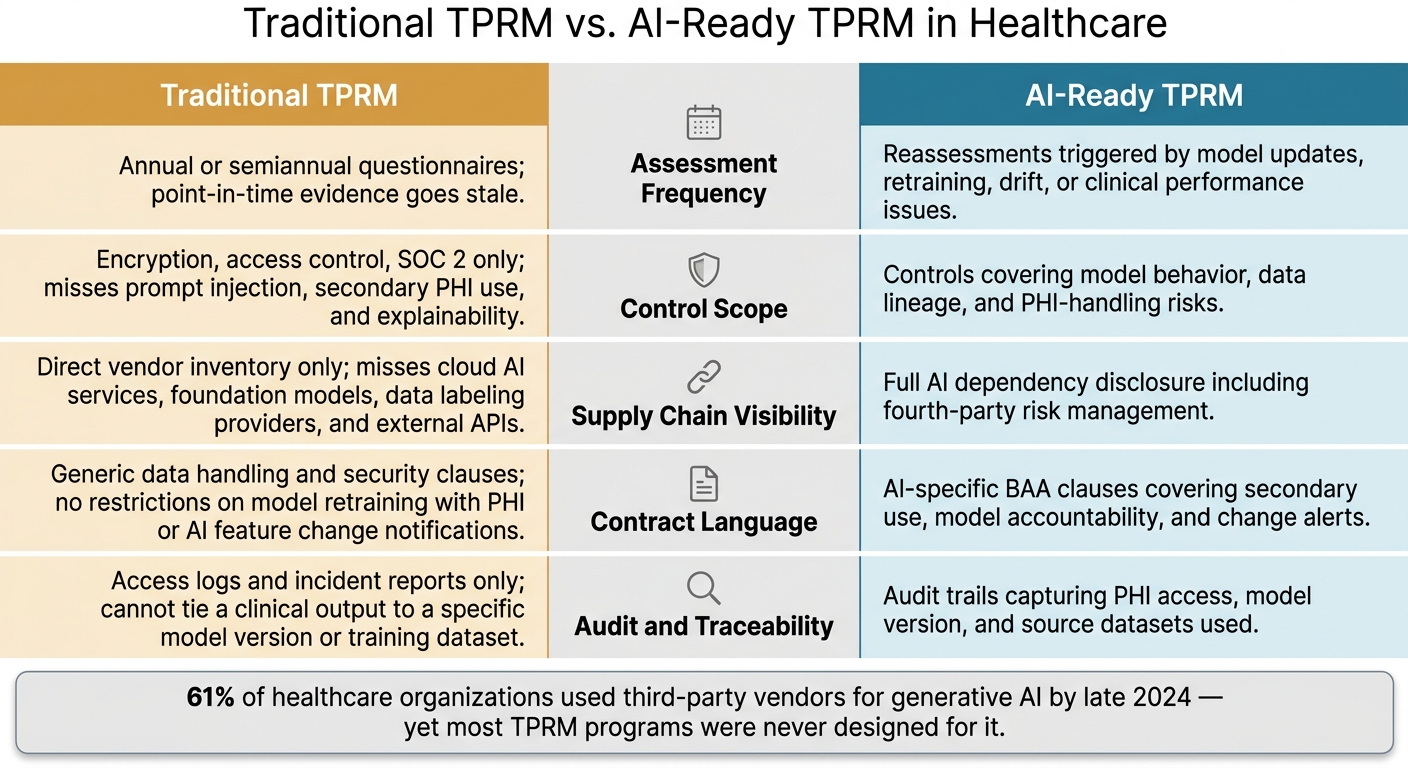
Traditional TPRM vs. AI-Ready TPRM in Healthcare: Key Gaps
Legacy TPRM assumes vendor systems stay pretty much the same between reviews. AI breaks that assumption.
In healthcare, that creates a serious problem. A vendor can change how it handles PHI, clinical outputs, or regulated workflows without setting off a new review. It might retrain a model, swap the training dataset, or turn on a new AI feature without sending a formal change notice [1][7][8].
In day-to-day use, the weak spots tend to show up in five areas. Here’s where the old approach runs into trouble:
| Process Area | Traditional Approach | Why It Fails for AI | AI-Ready Approach |
|---|---|---|---|
| Assessment Frequency | Annual or semiannual questionnaires | Point-in-time evidence goes stale | Reassessments triggered by model updates, retraining, drift, or clinical performance issues [1][4][6] |
| Control Scope | Encryption, access control, and SOC 2 | Misses prompt injection, secondary PHI use, and explainability | Controls covering model behavior, data lineage, and PHI-handling risks [7][8] |
| Supply Chain Visibility | Direct vendor inventory only | Misses cloud AI services, foundation models, data labeling providers, and external APIs | Full AI dependency disclosure, including fourth-party risk management [3][5][2] |
| Contract Language | Generic data handling and security clauses | No restrictions on model retraining with PHI or AI feature change notifications | AI-specific BAA clauses covering secondary use, model accountability, and change alerts [1][7][8] |
| Audit and Traceability | Access logs and incident reports | Cannot tie a clinical output to a specific model version or training dataset | Audit trails capturing PHI access, model version, and source datasets used [7] |
In healthcare, these gaps don’t stay on paper. They show up as missed PHI exposure, model changes that never got reviewed, and subcontractor dependencies hiding in the background.
Static Assessments Miss Model Drift, Retraining, and Feature Changes
Annual reviews made sense when software moved on a fairly predictable release cycle. AI doesn’t.
A vendor can retrain a model, change its training data sources, or roll out a new feature between assessments. The HSCC AI guide recommends at minimum annual revalidation for critical and high-impact AI systems, with added reassessments triggered by retraining events, model updates, new threat intelligence, or clinical performance issues [1].
That’s the main risk in plain English: a vendor passes review in January, changes the model in July, and your team is now relying on a system it never actually reviewed.
Opaque AI Supply Chains Create Fourth-Party and Data Lineage Blind Spots
Most vendor inventories stop at the company you signed the contract with. That sounds fine until you look under the hood.
An AI feature may rely on cloud AI services, foundation models, data labeling providers, or external APIs. Those are fourth-party dependencies. In healthcare, they create fourth-party risk and weak data lineage [3][5][2].
When that chain is hidden, it becomes much harder to figure out what failed, where it failed, and who owns the problem. It’s a bit like trying to trace a lab result without knowing which instrument ran the test.
Generic Security Controls Do Not Cover Generative AI, PHI Handling, or AI Behavior Risk
A SOC 2 report and other baseline checks can show that a vendor follows basic security hygiene. What they don’t show is just as important.
They do not tell you whether a generative AI tool keeps PHI in prompts or outputs, whether someone can manipulate outputs through prompt injection, or whether the model can explain its output in a way a clinician can review [7][8].
Put simply, baseline controls don’t deal with model behavior, PHI handling, or prompt injection. Standard questionnaires usually don’t ask about those issues, so they slide by unnoticed. That’s why vendor reviews need AI-specific questions, not just broader security checklists.
Those misses map straight to model lifecycle, privacy, and patient-safety risk.
AI-Specific Risks Healthcare Organizations Must Add to Vendor Reviews
Those gaps point to three AI review areas that need special attention: model lifecycle, privacy, and patient safety.
Model Lifecycle, Security, and Operational Reliability
Start with the model itself. Healthcare teams should review how the vendor handles model updates, retraining, and version changes. Ask for proof of change management for model updates, including whether customers get advance notice before changes go live in production. There should also be a documented rollback plan in case defects or safety problems show up.
The risk here isn't abstract. Security research shows that as few as 100–500 poisoned training samples can compromise a healthcare AI model and trigger targeted misclassifications, even while the model still looks normal in standard validation tests [9]. That’s why buyers should ask direct questions about how vendors vet training data sources, limit access to training pipelines, and watch for integrity problems after deployment.
It also helps to map each AI-dependent workflow by criticality. An AI tool that supports an admin task is one thing. An AI tool tied to care delivery is another. For that reason, require AI-specific SLAs, fallback workflows, and continuity plans that clearly name the AI component.
Model controls are only one piece of the review. The next issue is data handling.
Privacy, HIPAA Compliance, and Secondary Data Use
Track where ePHI enters, stays, and leaves the AI system. In practice, ePHI can show up in prompts, outputs, logs, embeddings, fine-tuning datasets, and analytics pipelines. Every one of those points can become an exposure path. Generative AI adds another layer of risk because it can leak or infer sensitive data, which means de-identification should be checked again before health data is used [11][10].
Secondary data use also needs a plain yes-or-no review. Vendors may use customer prompts, outputs, or fine-tuning data to improve general models used by other customers, and that often slips by without much scrutiny. Make sure there are explicit opt-in or opt-out controls. BAAs should also spell out limits on secondary use, data residency terms, and the full list of subprocessors that touch PHI or derived data.
Once the data picture is clear, the next step is to look at how the system shapes clinical decisions.
Bias, Explainability, and Patient Safety in Regulated Workflows
When AI influences clinical decisions, bias and explainability shift from technical issues to patient-safety issues.
Vendor reviews should ask for stratified performance metrics, not just a single top-line number. That means sensitivity, specificity, and false positive and false negative rates broken out by race/ethnicity, age, sex, and payer type where relevant. If a vendor can only show aggregate accuracy, that’s a gap. Performance differences across patient groups have been documented in AI tools used for imaging, risk scoring, and prior authorization, and regulators are watching more closely.
Explainability matters for a separate reason. If a clinician is expected to act on an AI output, they need enough context to judge it. Reviews should confirm that the system supports human-in-the-loop review, clearly signals uncertainty or low-confidence outputs, and includes documented escalation paths for ambiguous or high-risk cases. For high-impact use cases, document risk acceptance.
sbb-itb-535baee
How to Update TPRM for AI-Enabled Vendors
The fix is to treat AI as a standing trigger for review, not a one-time checkbox. AI vendors can change after approval through model updates, retraining, and new subprocessors. So TPRM has to move with them.
The flow is simple: identify the AI use case, lock it into the contract, then keep watch over it.
Update Intake, Due Diligence, and Governance for AI Use Cases
Every new vendor request and renewal should include an AI-specific intake section. Ask clear questions:
- Does the product use AI?
- What does the AI do?
- Which models does it use?
- Where do those models run?
- Which third parties support them?
Vendors should also provide an AI component inventory, sometimes called an AI bill of materials, plus architecture and data-flow diagrams. Those diagrams should show how PHI moves through the model, logs, and storage.
Risk tiering should account for PHI sensitivity and volume, clinical impact, and how much the AI acts without human review. A low-risk administrative tool does not belong in the same bucket as a clinical decision tool that acts on its own.
Intake flags like "uses PHI", "affects clinical decisions," and "uses external foundation models" should route the vendor to the right reviewers on their own. Low-risk tools can go through a lighter review path. Tools that affect diagnosis or treatment need cross-functional review, pilot monitoring, and cross-functional approval.
That same workflow should apply when an existing AI vendor makes material changes to its model, data, or subprocessors. Otherwise, feature expansion can slip through without review.
Once the AI use case is classified, the contract must lock those limits in.
Strengthen Contracts, BAAs, and Change Notification Requirements
BAAs need to spell out four points clearly. The covered entity should keep ownership and control of PHI. The vendor's use of PHI or derived data for model training or product improvement across its customer base should be limited. Any subprocessors and model providers with access to PHI should be named. And the vendor should give 30- to 60-day advance written notice before any material change to models, data, or subprocessors goes live, so the organization has time to reassess first. [12][14]
Once the contract sets the rules, monitoring has to show whether the vendor is following them in day-to-day use.
Move to Continuous Monitoring With AI-Specific Evidence and Telemetry
Continuous monitoring is what keeps AI-aware TPRM current between formal reviews. AI vendors should be monitored all the time, with reassessment triggered by model updates, retraining, new features, subprocessor changes, or AI incidents such as hallucinations or misclassifications that affect care. Event-driven reassessments should sit alongside scheduled periodic reviews, scaled to the vendor's risk tier.
Vendors should provide model version data, accuracy, false positive and false negative rates, drift signals, and clinician override rates. Healthcare AI monitoring frameworks point to at least four separate failure modes that need their own detection methods: performance drift, population drift, workflow drift, and version-change breaks. [13] Those signals help internal teams spot risk early instead of waiting for the next review cycle.
Teams should also keep a register of AI-related incidents. That register should include model failures, hallucinations, unexpected outputs, privacy events, misclassifications affecting care, and user escalations. Review it in governance meetings.
Putting AI-Aware TPRM Into Practice With Censinet
The hard part isn't defining AI-specific controls. It's turning them into a repeatable vendor-risk workflow that teams can use every time. At scale, AI-aware TPRM needs one place for intake, review, and monitoring.
Censinet RiskOps™ acts as that central hub. Risk teams can clearly tag AI-enabled vendors, attach AI-specific assessment templates, and keep supporting documents - like model cards, DPIAs, and SOC 2 reports - right in the vendor record. Censinet AI™ helps the review process move faster: it pulls out responses, maps them to controls, and flags gaps. For example, it can spot when de-identified clinical notes are sent to an external LLM without clear re-identification safeguards. It can also surface fourth-party AI exposure by finding signals in vendor documents that point to the use of external AI platforms. That gives risk teams a reason to ask for clarification, added contract terms, or security attestations before those relationships slip by untracked. RiskOps dashboards give governance teams a current view of AI risk across the vendor portfolio.
Once the AI inventory is set up, flagged risks can move to the right reviewers on their own. High-risk assessments route to the right people, such as the CMIO, compliance, or legal. Automation does the information synthesis. Accountable humans make the final call.
AI-aware TPRM works best when vendor data, governance review, and continuous monitoring stay connected. That setup helps healthcare teams review AI vendors the same way each time, document decisions clearly, and keep PHI, compliance, and safety controls current.
FAQs
What makes AI vendors riskier than traditional software vendors?
AI vendors can bring more risk because their systems often work like a black box. That makes security checks and data governance harder to confirm. And unlike static software, AI models can change over time. They can drift, or introduce bias that affects clinical outcomes.
There’s another issue: vendors may roll out AI features without telling you. That can create hidden dependencies and shadow AI before anyone spots the problem. Add in undisclosed fourth parties, weak de-identification, and threats like prompt injection, model poisoning, and unauthorized data training, and the risk picture gets messy fast.
When should an AI vendor trigger a new risk review?
A new risk review is needed any time there are material changes to the AI model or to the way it’s used.
Common triggers include:
- New AI features
- AI added after onboarding
- Changes to security, privacy, or contract terms that allow customer data to be used for LLM training
- Model retraining or drift
- Unusual API activity or behavior changes
What AI terms should be added to a BAA or contract?
Include contract terms that ban the use of protected health information to train AI models. Also require the vendor to disclose when AI is being used, where the training data came from, and how the model is governed.
The contract should also require notice before any material model update or retraining. On top of that, it should spell out who owns the data, give you audit rights, and extend BAA coverage to all downstream subprocessors.
