If a healthcare AI tool can affect care, billing, or patient data, I’d treat rollout and risk review as the same decision.
Here’s the short version: hospitals are putting AI into daily work faster than they are reviewing bias, accuracy, privacy, and billing risk. The article’s point is simple: if governance starts after purchase or after go-live, it starts too late.
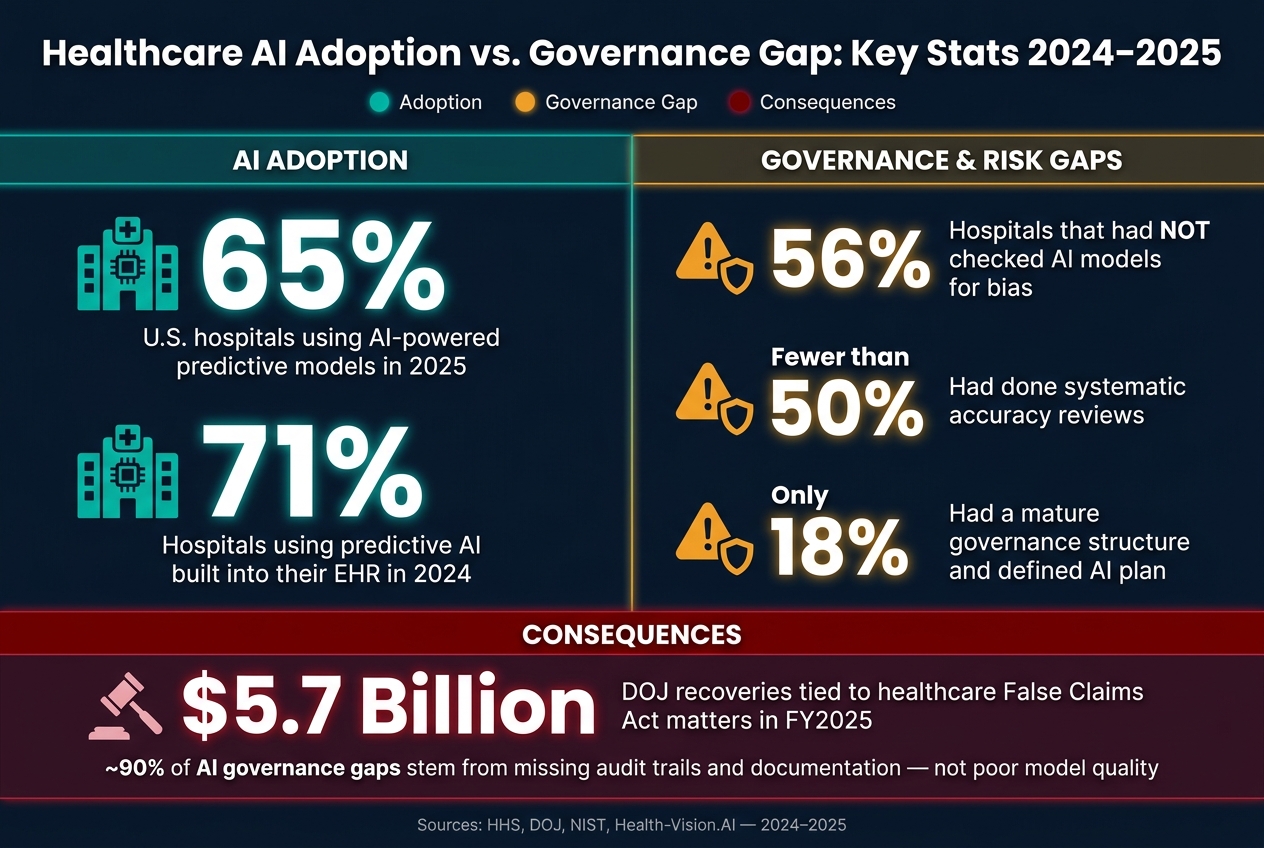
A few facts stand out:
- 65% of U.S. hospitals used AI-powered predictive models in 2025
- 56% had not checked those models for bias
- Fewer than half had done systematic accuracy reviews
- 71% of hospitals said in 2024 that they used predictive AI in their EHR
- Only 18% had a mature governance structure and a defined AI plan
- DOJ recoveries tied to healthcare False Claims Act matters topped $5.7 billion in fiscal year 2025
What I take from that:
- Clinical AI can put wrong or missing details into the medical record
- Diagnostic AI can slip in performance across patient groups or outside cleared use
- Revenue cycle AI can spread coding errors across thousands of claims
- Patient chatbots can mishandle PHI or give unsafe guidance
- Shadow AI can appear before legal, privacy, or security teams even know it exists
So the fix is not more meetings after rollout. The fix is to build one program that covers:
- AI inventory
- Risk tiers
- Vendor review
- Human review points
- Monitoring for drift and bias
- Audit trails
- Stop rules
- Incident response
- End-of-life shutdown
I’d sum up the article this way: healthcare AI should be approved, watched, and, if needed, paused under one shared decision model from day one. That means clinical, security, legal, compliance, procurement, and IT teams all have defined roles before the tool touches a patient, a claim, or PHI.
The rest of the piece supports that view with examples from ambient scribes, diagnostic support, billing tools, and patient-facing bots.
Healthcare AI Adoption vs. Governance Gap: Key Stats 2024–2025
Healthcare AI Governance - Risks, Compliance, and Frameworks Explained
sbb-itb-535baee
Where Healthcare AI Creates the Most Risk
Risk changes based on what the AI does and where it shows up in care. A scheduling assistant is one thing. A radiology triage tool is another. They do not carry the same exposure, so they should not go through the same review path.
The main idea is simple: match controls to the workflow. Adoption and risk review need to move together, and those workflow differences should shape the approval path before deployment.
The highest-risk workflows are the ones that enter the clinical record, affect a care decision, or shape a claim.
Ambient Documentation and Diagnostic Support Tools
Ambient AI scribes and diagnostic tools sit close to direct patient care, so they bring the most clinical risk. If an ambient documentation tool generates a clinical note, documentation mistakes or hallucinations can end up in the permanent medical record. That's why clinicians should require clinician attestation before a note is finalized.
Diagnostic support tools in radiology, cardiology, and pathology bring a different risk, but it's just as serious: algorithm drift. The FDA has authorized more than 950 AI-enabled medical devices, mostly in these specialties [2]. Each one is cleared for a specific clinical indication. If use drifts beyond that cleared indication or beyond the training data, performance can slip without much warning.
Bias makes this tougher. Diagnostic AI can perform unevenly across patient demographic groups. So teams need bias testing and post-deployment performance monitoring, not just a one-time review before launch.
Revenue Cycle Automation and Patient-Facing Chatbots
Revenue cycle AI works at scale. That's the upside, and it's also the danger. Coding, billing, and prior authorization tools can move through thousands of transactions fast. But when human oversight is weak, small errors can turn into large financial mistakes and billing compliance failures.
A few controls matter most here:
- Audit trails to track what the system did
- Human review checkpoints to catch billing and coding issues
- Reviews tied to payer rule changes and model drift
Patient-facing chatbots bring a different mix of problems. These tools handle scheduling, triage, and messaging. If PHI slips into external model training data, sensitive health information can be exposed. And if the bot gives inaccurate guidance or responds in a tone-deaf way, the damage can show up fast in both patient safety and public trust.
That is why content filters and triage override protocols are the minimum governance requirements for any patient-facing AI tool.
These controls should live inside the same rollout workflow as the AI tool itself.
Why AI Adoption and AI Risk Management Must Be One Program
The biggest failure point is simple: separate decision paths.
When strategy, security, privacy, compliance, clinical safety, and vendor risk all move on their own tracks, things break down fast. A tool can go live with open safety, privacy, or billing risk. Or it can be rolled out before anyone has settled a basic question: who gets to make the call when something goes wrong?
That’s why governance needs a defined operating model before the first deployment.
In 2024, 71% of hospitals said they were using predictive AI built into their EHR, but only 18% had a mature governance structure and a fully formed AI strategy [5]. That gap says a lot. Adoption is moving ahead. Governance often isn’t.
And this isn’t mainly a technical controls issue. You can have encryption, access logs, and vendor contracts in place and still be stuck on a very human question: Who has the authority to pause this tool if it starts behaving unexpectedly? That’s not a tooling problem. It’s an organizational design problem.
The answer is a single operating model that ties together AI strategy, cybersecurity, privacy, compliance, clinical safety, and vendor risk under one governance structure. Not a handful of separate workstreams that meet now and then. One program. Shared accountability.
Build a Healthcare-Specific AI Governance Framework
Healthcare AI needs more than an acceptable use policy. Clinical AI, administrative AI, and shadow AI do not carry the same level of exposure, so they should not be handled the same way.
A working framework needs a few core parts:
- An AI inventory
- Risk tiers
- Lifecycle stages
- Alignment to recognized standards
Two frameworks matter most right now. The NIST AI Risk Management Framework (AI RMF) covers operational risk and trustworthiness. ISO/IEC 42001 focuses on maturity and audit readiness. More healthcare organizations are lining up with both so they can build one compliance posture instead of patching things together [3].
There’s also a policy shift worth watching. A December 2024 proposed rule from HHS would require covered entities to keep a documented technology asset inventory and complete a written risk analysis at least once a year, with AI systems named directly in that scope [2].
One line the framework must draw very clearly: clinical AI is not the same as administrative AI.
A diagnostic support tool used with a high-acuity patient carries a very different risk profile - and a very different regulatory burden - than a scheduling assistant. Risk tiering should reflect that. The higher the stakes, the tighter the oversight.
The framework also has to deal with shadow AI. These are tools clinicians or staff start using without formal review. That creates undocumented HIPAA and clinical risk, and no policy document will catch that by itself. Network-level visibility and endpoint monitoring are practical controls that can help surface this kind of exposure [2].
Once the framework is in place, ownership needs to be assigned across clinical, technical, legal, and risk leaders.
Assign Decisions to a Multidisciplinary Governance Team
Governance falls apart when the right people aren’t in the room. You end up with policies that sound fine on paper but don’t survive contact with day-to-day care delivery.
The team reviewing AI use cases should include CISOs, CIOs, clinical informatics leads, legal, compliance, quality management, and procurement. Just as important, each group needs clear decision-making roles. This team owns approval, escalation, and stop authority.
The table below maps each NIST AI RMF function to the owner and what they own:
| NIST AI RMF Function | Owner | Accountability Focus |
|---|---|---|
| GOVERN | Executive leadership, CISO, Legal | Defining risk tolerance, decision rights, and escalation paths |
| MAP | Clinical leads, Compliance, IT | Identifying affected populations, error types, and outcome boundaries |
| MEASURE | Clinical Informatics, Data Science | Continuous performance monitoring and subgroup stratification |
| MANAGE | Risk Management, Clinical Oversight | Proactive risk treatment, residual risk decisions, and system retirement |
Procurement should be part of this group from the start, not pulled in at the contract review stage. A lot of AI risk gets shifted through vendor agreement language tied to audit rights, indemnification, and data use [3].
The team also needs defined stop conditions. In plain English, that means clear criteria for when a tool can move forward, when it needs more review, and when it should be paused or retired. Those thresholds make lifecycle reviews far less fuzzy, and they carry straight into risk assessment, monitoring, and incident response.
How to Put AI Risk Management Into Practice Across the Lifecycle
Once governance roles and decision rights are set, the next step is day-to-day execution. In healthcare, that means using repeatable controls before purchase, during deployment, and through monitoring and shutdown. The controls below turn governance from a policy on paper into routine operating practice.
Start with AI Risk Assessments and Vendor Due Diligence
A pre-purchase AI risk assessment should spell out the intended use, PHI exposure, patient safety and operational impact, and the evidence a vendor can share on validation results, monitoring plans, and rollback procedures before deployment [2][6].
AI-focused due diligence should ask for model training and validation details, data provenance, bias mitigation strategies, and PHI/PII redaction methods [1][6]. Vendors should also be able to provide an AI bill of materials, or AIBOM, showing model dependencies, open-source components, APIs, and any downstream dependencies that may bring hidden risk [1].
Contracts need to match those risks. Business Associate Agreements (BAAs) should be updated to bar the use of PHI to train public models and to set AI-specific breach notification timelines [1][2].
Apply Data Controls, Human Oversight, and Model Monitoring
Once a model is approved, it should be controlled like any other ePHI-bearing system. Technical controls should meet the same HIPAA requirements used for any ePHI system, including access controls, audit logging, and transmission security [2].
AI adds another layer. Teams should version prompts and datasets, trace each output back to a model version, and keep rollback capability in case a model update hurts performance [6]. That traceability matters. If something goes sideways, you need to know which version did what.
Human oversight should also be built into clinical and other high-impact workflows. That means:
- Named oversight owners for each use case
- Defined override mechanisms
- Clear escalation workflows when a clinician disagrees with an AI output [4][6]
Continuous monitoring should use subgroup stratification too, so average accuracy scores do not mask bias or weaker performance in certain patient populations [4].
The table below maps key post-deployment control areas to practical actions:
| Control Category | Post-Deployment Action | Alignment |
|---|---|---|
| Data Access | MFA, encryption, audit logging | HIPAA Technical Safeguards |
| Monitoring | Continuous drift detection and subgroup stratification | NIST MEASURE Function |
| Oversight | Named clinical owners, override rights, escalation workflows | NIST GOVERN Function |
| Change Management | Documented asset inventory and FDA PCCP tracking | HIPAA Administrative / FDA Regulatory |
Plan for AI-Specific Incidents and Lifecycle Oversight
Monitoring only helps if teams can pause or roll back a failing system fast. AI incidents can include hallucinations, model drift, biased outputs, data leakage, and vendor failures. Those risks need response plans that go beyond standard breach protocols [4].
Incident response plans should define explicit triggers for each failure mode [4]. Stop conditions should be written down before deployment, not after an issue appears. These are predefined performance thresholds that trigger an immediate pause [4]. For example, if a false negative rate goes above a set threshold over 30 days, that should automatically escalate to the governance team for a suspension decision [4].
"The question is not whether the organization can respond after a patient harm event; it is whether the organization has the governance infrastructure to respond to a performance signal before it becomes a harm event." - Brian M. Green, M.S., Chief AI Officer & Founder, Health-Vision.AI [4]
Risk management also needs to continue through termination. End-of-life plans should require data destruction and vendor offboarding so leftover exposure is closed out [1].
Conclusion: Responsible Healthcare AI Requires Integrated Governance from the Start
AI in U.S. healthcare has moved past the pilot stage. It now shows up in clinical care, billing, and patient communications. And each deployment choice carries real stakes for patient safety, PHI, compliance, and organizational liability. The main point is straightforward: AI governance must start before deployment.
In fiscal year 2025, the U.S. Department of Justice recovered more than $5.7 billion tied to healthcare False Claims Act matters [7]. In 2026, Pennsylvania sued Character.AI after its chatbots allegedly posed as physicians and gave users fake medical license numbers [7]. Those cases show what happens when AI moves faster than oversight. Governance can't be added later like a patch.
In healthcare, AI is a governance issue before it's anything else. So the practical move is to make governance part of the rollout itself.
That means building it into each stage of deployment: assess risk before purchase, assign decision rights, put data controls and human oversight in place at launch, and keep watch through retirement. In healthcare, adoption and risk management are one process - not two separate tracks. That's the kind of discipline that makes scale possible.
About 90% of AI governance gaps in health systems come from missing evidence, including audit trails and documentation, not poor model quality [6]. Organizations that put traceability, clear oversight, and stop authority in place from day one are in a stronger position to scale with care, meet regulatory demands, and protect patients.
FAQs
What counts as high-risk healthcare AI?
High-risk healthcare AI covers any tool or feature that can shape diagnosis, treatment, reimbursement, clinical decision support, consent, or patient understanding. It can also include coding, billing, and recommendations shown directly to patients.
These uses need tighter oversight because they can affect patient safety and regulatory compliance. A small error here isn’t just a technical glitch. It can change care decisions, confuse patients, or create compliance problems.
That’s why organizations should sort AI systems by risk level and apply stronger controls where the stakes are higher. In practice, that often means:
- Human review before or during use
- Bias audits to check for uneven results across groups
- Performance monitoring to track how the system behaves over time
The main idea is simple: the more an AI system can influence care or payment, the more closely it should be watched.
Who should approve and monitor AI tools?
Healthcare organizations should use a cross-functional AI governance committee to review, approve, and track AI tools. That group should include clinical leadership, information security, compliance, legal, data science, product, and engineering.
Clear accountability matters. Each part of the process should have a named owner, including risk assessment, deployment approval, and ongoing monitoring. Clinician involvement is a must because it ties technical work directly to patient safety across the full AI lifecycle.
How can hospitals find shadow AI early?
Hospitals can spot shadow AI earlier if they have better visibility into network activity and day-to-day operations. One practical move is to use egress proxies or HTTP enforcement layers to detect and route traffic going to known AI service endpoints and vendor SaaS APIs.
It also helps to watch for AI-assisted clinical documentation patterns. On top of that, data loss prevention tools can flag protected health information sent to unapproved destinations. That matters because a busy clinician may not realize where sensitive data is going once it leaves an approved system.
Just as important, pair those controls with a fast, governed AI procurement pathway. If security review takes too long, staff will often look for shortcuts, and that can disrupt clinical workflows instead of supporting them.
