Cybersecurity change in healthcare often fails for one simple reason: staff see new controls as extra work that gets in the way of care. ISO 27001 helps fix that by giving teams a clear way to assign ownership, document risk, explain decisions, train staff by role, and review changes after rollout.
If I had to sum up the article in a few points, it would be this:
- Resistance usually starts with workflow friction, like MFA, VPN logins, and access requests slowing down care
- Weak governance makes pushback worse, especially when no one knows who approved a control or why
- ISO 27001 reduces that friction through defined roles, leadership accountability, risk assessment, treatment plans, and staff communication
- Change works better when tied to the risk register, not handled as a stand-alone IT ticket
- Teams should track adoption with simple measures, like training completion, exception volume, incident response time, and the mix of standard vs. emergency changes
- Paper-only programs fail, especially when clinical teams are left out
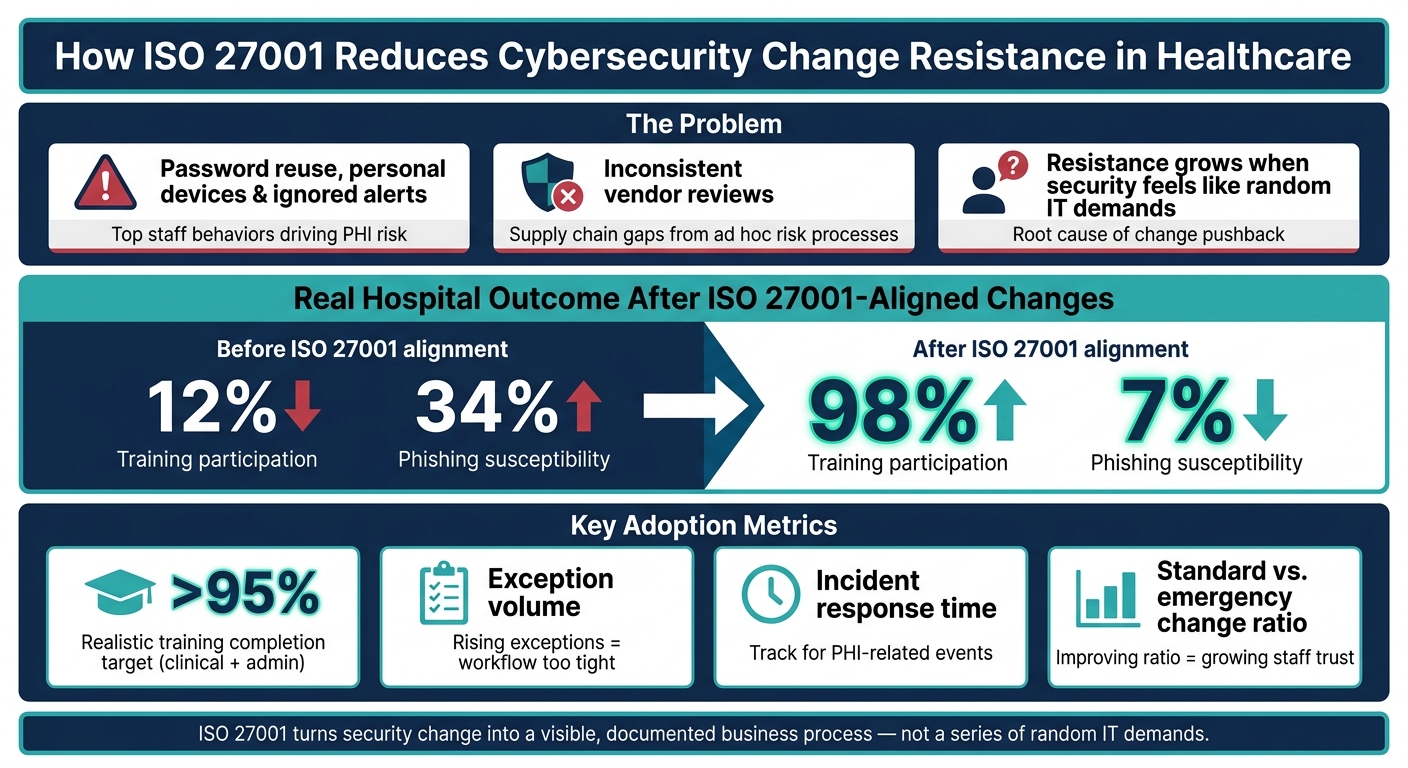
The article also points to a few hard numbers that matter. PHI breaches are expensive, training targets above 95% are realistic, and one hospital saw training participation move from 12% to 98% while phishing susceptibility dropped from 34% to 7% after ISO 27001-aligned changes.
What I take from this is simple: people resist controls they don’t understand, don’t trust, or had no role in shaping. ISO 27001 helps by turning security change into a visible, documented business process instead of a series of random IT demands.
That’s the core idea behind the full piece.
ISO 27001 in Healthcare: Key Stats & Outcomes
The problem: what drives resistance to cybersecurity change
Cultural and operational barriers
Cybersecurity change tends to stall when it adds friction to clinical work. If an MFA prompt slows access to a patient record, or a VPN login holds up care delivery, staff usually don’t see a safeguard. They see a roadblock.
A lot of employees still treat cyber risk like someone else’s problem. That mindset leads to password reuse, personal devices being used to access PHI, and alerts getting ignored [1]. And when governance is uneven, fixing that friction gets even harder.
Weak governance and ad hoc risk processes
Things get worse when there’s no clear decision process. Resistance grows when cybersecurity is handled like an IT-only task instead of a shared responsibility across the organization. If security decisions happen inconsistently, risk registers sit untouched, and no one is sure who owns what, new controls can feel random. Staff don’t know who made the call, why it happened, or how it ties back to their day-to-day work.
"Your MSP can't get you certified, because it was never an IT project to begin with." - Ben Carrick, Strategist, LeftBrain [4]
You can see the same issue in vendor management. Healthcare organizations often deal with dense vendor networks. Without a repeatable risk process, those vendor relationships get reviewed in uneven ways - or not reviewed at all. That leaves healthcare supply chain security challenges that are much harder to fix later [5].
Why staff push back when the business case is unclear
Technical language rarely wins over clinical staff. If the reason for a control doesn’t connect to their work, the change feels forced instead of useful.
Adoption gets better when leaders explain security changes in terms staff already care about, like keeping systems up during a shift, protecting patient records, and avoiding disruption to daily operations. The case for change has to connect to patient care and the work happening on the ground.
ISO 27001 helps here by making security decisions visible, repeatable, and easier to explain.
sbb-itb-535baee
How ISO 27001 reduces resistance through structure and transparency
ISO 27001 lowers friction by making change visible, owned, and easy to explain.
Context, leadership, and defined responsibilities
Cybersecurity work often stalls when no one knows who owns what. ISO 27001 helps fix that by assigning responsibility early through its leadership, planning, and responsibility requirements. That gives clinical leadership, compliance, IT, and operations a clearer part in the process [1][5].
Leadership commitment under Clause 5 matters a lot. When executives follow the same controls as staff, pushback tends to drop [1][6]. And when staff help shape policies and workflows, adoption usually goes more smoothly.
With roles spelled out, risk decisions and vendor risk assessment processes are also easier to defend.
Risk assessment and treatment that make change easier to justify
ISO 27001's Clause 6.1.2 requires a documented, repeatable risk assessment method. That moves decisions away from case-by-case judgment and toward documented business impact [1][5].
The Statement of Applicability shows why each control is included or excluded. For clinical and operations teams, that gives a plain reason for the change. This clarity is especially helpful when teams are tasked with answering security questionnaires that justify their internal controls. It makes the work feel tied to an actual risk, not a random rule [5].
That point matters even more for medical devices that can't be patched. If those limits are documented in the risk treatment plan, along with compensating controls, teams get a clear answer to the usual "why are we doing this?" frustration that slows rollouts [5].
After the "why" is on paper, staff still need a simple and steady way to take in the change.
Training, communication, and awareness built into the standard
ISO 27001 supports role-based, frequent training that staff can absorb more easily. Plain-language communication also helps people adopt controls faster [1].
"If people can't understand security, they can't follow it. ISO 27001 succeeds when communication is clear, not impressive." - Canadian Cyber [1]
These controls tend to work best when they fit into daily risk workflows instead of being treated like one-time projects.
Putting ISO 27001 into practice in healthcare risk programs
Embed change management into cybersecurity projects
Once ISO 27001 is in place, the next move is to work it into day-to-day change control. This is where many teams hit a snag. Controls may look solid on paper, but the friction shows up when people start using them in live settings. Rolling out MFA for EHR access or segmenting clinical networks can interrupt daily work if there isn't a clear process behind the change.
The fix is simple in principle: treat each change as a risk decision, not just an IT task.
Link every change request to the risk register so higher-impact changes go to review based on risk rating [3]. That gives clinical and operations leaders a clearer view of what's being proposed and why it matters.
For routine, low-risk work such as SSL certificate renewals, use a pre-approved standard change workflow. That keeps the Change Advisory Board focused on the changes that need close attention [3]. For higher-risk changes, stick to a short, plain lifecycle:
- Initiate
- Assess risk
- Approve
- Test
- Implement with rollback
- Review
Review each change two weeks after go-live. That short follow-up window helps teams spot unintended effects early.
"The goal is a clear, enforceable policy that integrates with daily operations. The biggest mistake I see? Policies that are either too vague or so complex they become shelfware." - Nojus Bendoraitis, General Counsel, Copla [3]
Use Censinet RiskOps™ to run ISO-aligned risk workflows
A central risk platform can take a lot of the drag out of this work, especially at scale. Censinet RiskOps™ brings ISO-aligned risk assessments, evidence, and approvals into one place across IT, compliance, clinical operations, and vendors.
That matters because risk work in healthcare rarely sits with one team. It cuts across departments, and without one system of record, things can get messy fast.
"Effective ISO 27001 implementation happens when information security is treated as a business enabler, not a compliance checkbox." - Gary O'Brien, CEO & Co-Founder, Safe Harbour Security [2]
Measure adoption and trust over time
Teams also need to check whether the process is making work smoother, not just producing more documentation. The best signals are practical ones: assessment cycle time, culture of cybersecurity training completion rates, policy exception volume, and incident response time for PHI-related events [3] [7] [8].
A target of over 95% training completion across clinical and admin teams is realistic [8]. If exception volume starts climbing, that often points to a workflow that is too tight for daily use. In many cases, the process needs tuning more than the staff need blame.
Another useful signal is the ratio of standard changes to emergency changes over time [3] [2]. When that ratio improves, it's often a sign that staff trust the formal process enough to use it instead of working around it.
Common pitfalls and how to sustain lower resistance
Avoid treating ISO 27001 as a paperwork exercise
ISO 27001 tends to fall apart when teams treat it as an IT-only project.
If policies are written without clinical input, staff often push back in quiet ways. They create workarounds, adoption drops, and the gap between policy and day-to-day care gets bigger. And when leaders ignore the same controls they expect everyone else to follow, people don't see the program as part of how work gets done. They see red tape.
The pattern is pretty simple: people push back on systems they had no hand in shaping.
In healthcare, that issue gets even tougher because exceptions are part of the job. Some devices still run software that can't be patched, which means teams need documented compensating controls [5].
The way to keep resistance lower is less glamorous, but it works: shared ownership, steady review, and governance that can hold up even when staff roles change.
Key takeaways for healthcare leaders
These pitfalls point to one clear idea: adoption lasts only when ISO 27001 becomes part of daily operations.
Resistance to cybersecurity change in healthcare usually doesn't come from bad intent. More often, it comes from unclear purpose and poor process design. If staff don't know why a control exists, or how it fits the way they actually work, they'll check out - or work around it.
ISO 27001 helps cut that friction because it gives teams a steady structure. That includes defined roles, documented risk methods, built-in communication requirements, and a continuous review cycle. In one hospital, ISO 27001-aligned changes lifted training participation from 12% to 98% and cut phishing susceptibility from 34% to 7% [9].
For healthcare leaders, a few habits matter most:
- Bring clinical stakeholders in early
- Roll out changes in phases
- Use plain language in every part of the program
Censinet RiskOps™ can support ISO-aligned risk assessments and collaborative risk management over time, so the program stays a working system instead of turning into a paper exercise.
FAQs
How does ISO 27001 reduce staff pushback?
ISO 27001 can cut staff pushback by making cybersecurity a shared job instead of another rule handed down from the top. When clinicians, IT teams, and other stakeholders are brought in early, the end result is usually a better fit for day-to-day work.
That matters a lot in healthcare. If a process looks good on paper but slows people down in practice, people will resist it. Early input helps shape workflows around what staff can actually use.
Clear language helps too. So do short training sessions and steady feedback. Those small choices make changes easier to grasp and less disruptive to clinical routines.
Censinet RiskOps™ can also lighten the assessment load. That means staff can keep their attention on patient care and avoid the drag of constant change fatigue.
Which healthcare teams should be involved first?
To cut resistance to change and help the project move forward, bring in a cross-functional team from day one. That should include leadership, IT, security, compliance, clinical operations, procurement, and vendor management.
Getting these groups involved early brings more perspectives to the table and helps break down silos. It also makes it easier to show that information security isn't just an IT issue - it supports patient care and day-to-day efficiency across the organization.
Clear roles and responsibilities matter too. They reduce confusion, keep decisions moving, and make accountability much stronger.
How can we tell if security changes are being adopted?
Use a formal change-review process to track day-to-day use and catch configuration drift early. Regular stakeholder meetings also help keep key risk indicators and performance metrics in view.
Set clear success criteria, then review change records to confirm updates were carried out as planned and met their goals. Feedback from front-line teams can help confirm that new workflows are being used in day-to-day work.
