If patient records, devices, or ordering systems go down, the issue is no longer just about IT. I’d sum it up like this: cyberattacks can trigger HIPAA, CMS, FDA, and state-law scrutiny at the same time, especially when care is delayed or records are incomplete.
Here’s the short version:
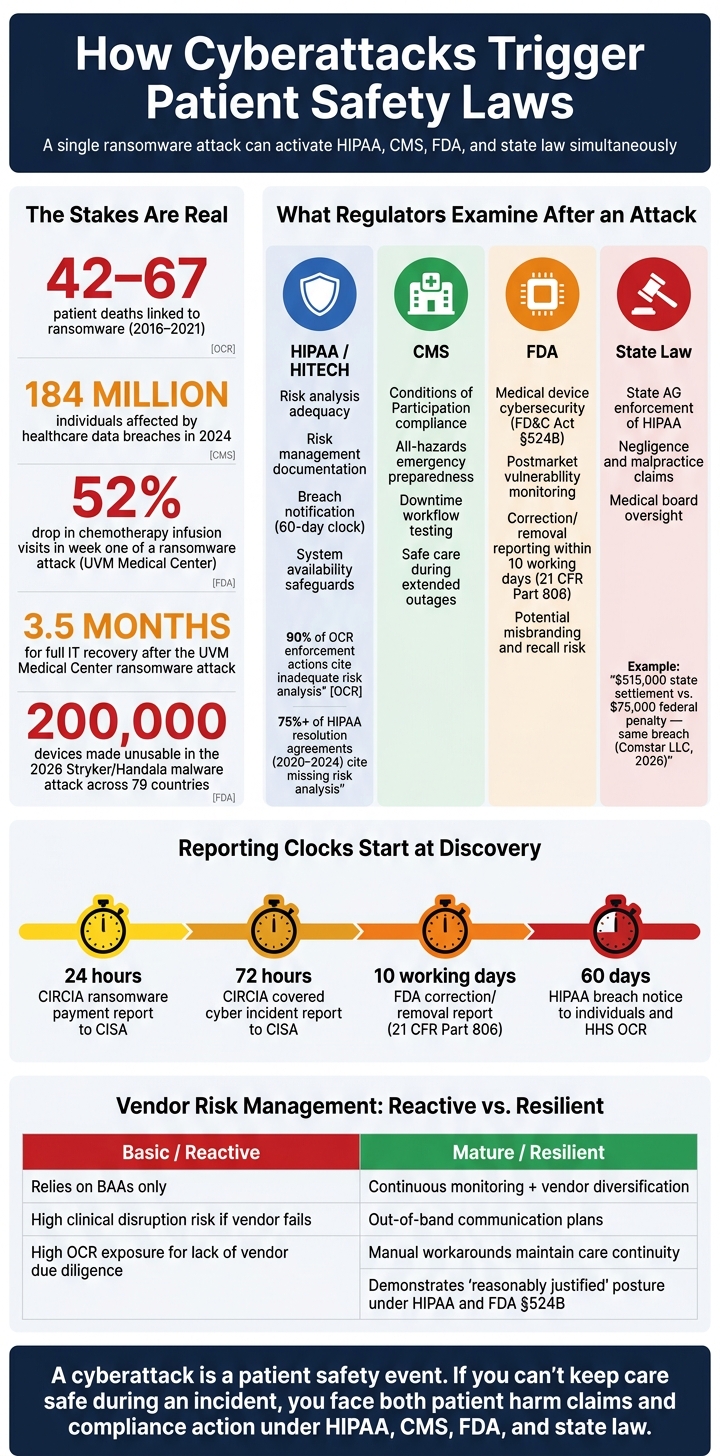
- Patient harm is part of the legal risk. Research cited here links ransomware to 42 to 67 patient deaths between 2016 and 2021.
- Regulators look backward after an attack. They often ask whether the provider had a documented risk review, tested downtime plans, and working safeguards before the incident.
- HIPAA risk review failures show up often. The article notes that weak or missing risk analysis appeared in 90% of OCR HIPAA Security Rule enforcement actions.
- Care delays create legal exposure. If EHRs, pharmacy tools, imaging, or connected devices fail, diagnosis, treatment, and charting can all suffer.
- Vendors can spread the damage. A third-party outage can still leave the hospital on the hook.
- Reporting clocks start early. Different rules can require notice in 24 hours, 72 hours, 10 working days, or 60 days, depending on what happened.
What matters most is simple: if you can’t keep care safe during a cyber incident, you may face both patient harm claims and compliance action.
| Area | What a cyberattack can trigger |
|---|---|
| HIPAA / HITECH | Review of risk analysis, risk management, breach notice, and system availability |
| CMS | Review of downtime planning, safe care during outages, and emergency preparedness |
| FDA | Device cybersecurity, corrections or removals, and postmarket duties |
| State law | Attorney General action, negligence claims, and board oversight questions |
So when I look at this article as a whole, the message is clear: healthcare organizations need cyber response plans built around safe patient care, not just system recovery.
Cyberattack Compliance Triggers: HIPAA, CMS, FDA & State Law at a Glance
Cyberattacks on Hospitals Are Attacks on Communities: Why Ransomware Is a Patient Safety Crisis
sbb-itb-535baee
U.S. Patient Safety Laws and Regulations That Cyberattacks Can Trigger
A ransomware attack can set off HIPAA, CMS, FDA, and state-law duties at the same time. That’s why it helps to know what applies before a regulator starts asking questions.
HIPAA, HITECH, and OCR Expectations for System Availability and Risk Analysis
The HIPAA Security Rule (45 CFR 164.308) requires safeguards for the confidentiality, integrity, and availability of ePHI. So when a cyberattack knocks systems offline, OCR looks closely at whether the organization saw those risks coming and took steps to deal with them.
That issue shows up again and again in enforcement. Inadequate risk analysis has appeared in 90% of all OCR HIPAA Security Rule enforcement actions [7]. Failure to conduct an adequate organization-wide risk analysis was also cited in more than 75% of HIPAA resolution agreements involving security incidents from 2020 to 2024 [9]. In plain terms, if an organization can’t show where ePHI lives, what could go wrong, and what it did about it, that becomes a major problem fast.
As OCR Director Paula M. Stannard has stated:
"A HIPAA risk analysis is essential for identifying where ePHI is stored and what security measures are needed to protect it. Completing an accurate and thorough risk analysis that informs a risk management plan is a foundational step to mitigate or prevent cyberattacks and breaches." - Paula M. Stannard, Director, HHS Office for Civil Rights [7]
Starting in 2026, OCR expanded its Risk Analysis Initiative to also scrutinize Risk Management. That means regulators now want proof that known risks were actively addressed, not just listed in a document [7]. And timing matters: the 60-day breach clock starts at discovery, so forensic work does not pause reporting [9].
CMS Conditions of Participation and Emergency Preparedness Duties
Hospitals that take part in Medicare and Medicaid must meet CMS Conditions of Participation (CoP), including all-hazards emergency preparedness planning. CMS guidance directly ties cyberattacks to shutdowns in clinical operations and threats to continuity of care [6].
If a long outage forces patient diversions or stops a hospital from providing services, CMS surveyors don’t look only at whether the servers came back. They look at whether the hospital kept the care setting safe while systems were down. That’s a different standard, and it matters.
CMS and The Joint Commission now assess whether hospitals can keep care safe during extended outages, not just restore systems quickly [6].
When outages spread to connected devices, FDA and state-law duties can enter the picture too.
FDA Rules, State Liability, and Board Oversight Obligations
Connected devices pull FDA rules into scope. FD&C Act Section 524B requires device manufacturers to monitor and address postmarket cybersecurity vulnerabilities. If they don’t, FDA can issue warning letters and civil penalties [8]. If a cybersecurity fix cuts a health risk, reporting is due within 10 working days under FDA 21 CFR Part 806 [8]. FDA may also view weak cybersecurity labeling as misbranding, which can lead to recalls [5].
State enforcement adds another layer of exposure. Under the HITECH Act, State Attorneys General have their own power to enforce HIPAA and can investigate at the same time as OCR, often with steeper penalties. In January 2026, the Attorneys General of Massachusetts and Connecticut reached a $515,000 settlement with Comstar LLC, an ambulance billing business associate, after a 2022 ransomware attack. The federal OCR penalty for that same breach was $75,000, bringing total exposure to $590,000 [7]. That spread shows how state action can outpace federal penalties for the same breakdowns.
Boards and executives are under more scrutiny too. Regulators now expect governance-level accountability for enterprise risk and patient safety. When oversight is weak, cyber risk can turn into clinical risk. Put simply, boards need to treat cyber risk as part of patient safety, not as an IT-only issue.
Those duties come into sharp focus when a cyberattack delays care, disrupts documentation, or makes treatment unsafe.
How Cyberattacks Cause Patient Harm and Raise Legal Exposure
Clinical Outages That Delay Diagnosis, Treatment, and Documentation
When clinical systems go down, the damage isn’t limited to IT. Orders take longer, records vanish from view, and the odds of patient harm go up. At the same time, those outages leave behind missing or patchy documentation, which can become a major problem when regulators review compliance.
The University of Vermont Medical Center lived through exactly that. A ransomware attack shut down chemotherapy infusion technology and took electronic health records offline. Infusion visit volume fell 52% in the first week, and full IT recovery took 3.5 months. Nurses had to document care by hand, and those incomplete records can make it harder to show risk analysis and downtime response during review [8][4].
Ransomware attacks can also force delays in elective procedures, ambulance diversions, and, in severe cases, deferrals of critical care, including cancer treatment [10]. And incomplete records aren’t just a sign of a bad week. They can also make OCR investigations harder to navigate [10][1].
Compromised Medical Devices and Unsafe Care Environments
Connected medical devices create a different kind of patient safety problem. If a cyberattack disrupts those systems, care teams may need to fall back on manual bedside monitoring and manual verification of device output until service is restored [8].
That stopgap matters even more when the device can’t simply be disconnected without putting a patient at risk. A ventilator is the clearest example. In cases like that, manual verification becomes a key safety step [8].
Third-Party and Supply Chain Failures That Spread Operational Risk
Vendor outages can turn a cyber incident into a supply-chain mess fast. In March 2026, a destructive malware attack tied to the group Handala hit Stryker Corporation’s Microsoft Intune environment. The attackers sent factory reset commands that made an estimated 200,000 devices across 79 countries unusable. Patient-facing devices stayed safe, but the attack wiped out electronic ordering systems. Hospitals ended up relying on phone calls and spreadsheets to find orthopedic implants and surgical tools for scheduled procedures [11].
Healthcare organizations can’t hand off blame for this kind of failure. Under HIPAA, they still own responsibility for third-party risk at the vendor level [12]. That matters because attackers are going after business associates and third-party vendors more often; one weak point can open the door to several healthcare networks at once. In 2024 alone, healthcare data breaches affected 184 million individuals [12].
| Control Approach | Patient Safety Impact | Regulatory Exposure |
|---|---|---|
| Basic (Reactive): Reliance on written Business Associate Agreements (BAAs) only. | High risk of clinical disruption if a single-source vendor fails [11]. | High; OCR views lack of vendor due diligence as a failure of the Risk Analysis requirement [1][12]. |
| Mature (Resilient): Continuous monitoring, vendor diversification, and out-of-band communication plans. | Lower risk; manual workarounds and alternative suppliers help maintain continuity of care [11]. | Lower; shows a forward-looking, "reasonably justified" posture under HIPAA and Section 524B [8][12]. |
How Healthcare Organizations Can Stay Compliant During and After an Incident
Build Incident Response Around Patient Safety, Not Just Technical Recovery
Once a cyberattack disrupts care, compliance comes down to one thing: can the organization keep patients safe while systems come back online?
Hospitals need to show which systems and workflows are safe to restore before care resumes. That means response plans can't focus only on getting servers back up. They need to protect clinical continuity first. Downtime workflows should be built by service line, including ED triage, pharmacy, radiology, and surgery scheduling. A clinical lead should sign off on restored data before it moves back into care workflows. Teams also need clear escalation thresholds ahead of time. Specific patient-safety triggers - such as when to divert ambulances, cancel surgeries, or transfer patients - should be documented and agreed on before an incident happens [6].
That operational work needs to be backed by fast, well-kept reporting.
Document Reporting, Root Cause Analysis, and Corrective Action Thoroughly
When a cyber incident starts, several reporting clocks start ticking at the same time.
CIRCIA requires reporting a covered incident to CISA within 72 hours and any ransomware payment within 24 hours. HIPAA requires notice to affected individuals and HHS OCR within 60 days of discovering a breach. FDA 21 CFR Part 806 requires reporting a correction or removal within 10 working days if it is needed to reduce a health risk [8]. If reporting is delayed, safety gaps can stay hidden, and corrective action can stall.
CMS and Joint Commission rules also require tested downtime workflows, reconciliation plans, and defined escalation thresholds [6]. During the incident, teams should document a clinical impact analysis that connects the exploit pathway to possible patient harm, shows how backup controls performed, and records the residual risk [8].
That record should then feed a root-cause analysis and, when needed, a corrective-action record inside the organization's Quality Management System [8].
Align Enterprise, Vendor, and Device Risk Management With Patient Safety Goals
Recovery doesn't rest only on the healthcare organization. Vendors and device partners have to show they're ready too.
A vendor failure can spill straight into clinical disruption. Because of that, business associate contracts should require proof of recovery and restoration testing, not just incident notice [6]. If a vendor can say it was attacked but can't produce backup integrity logs or show a tested recovery point, the covered entity is still exposed under HIPAA's risk analysis rules [6][8].
When teams use Censinet RiskOps for healthcare to document enterprise, vendor, and device risk, they can also show regulators that patient safety drove the response.
Conclusion: Cyber Resilience Is Now Part of Patient Safety Compliance
Put it all together, and the message is plain: a cyberattack is now a patient safety event, not just an IT issue. When systems go down, care can be delayed, devices can stop working as expected, and legal exposure can follow under HIPAA, CMS, FDA, and state law.
Under the proposed 2026 HIPAA Security Rule update, controls such as MFA and network segmentation would require technical enforcement [3][2].
For healthcare organizations, that points to three clear priorities: continuous risk assessment, tested downtime procedures, and vendor and device governance that regulators can verify [3][2].
Censinet RiskOps™ helps healthcare organizations centralize third-party and enterprise risk assessments in one workflow.
Cyber resilience is now part of patient safety compliance.
FAQs
What makes a cyberattack a patient safety issue?
A cyberattack turns into a patient safety issue when it disrupts clinical work and puts care at risk. It can block access to electronic health records, interfere with medical devices, and delay urgent treatment or emergency procedures.
When systems go offline, staff often have to switch to manual workarounds. That can increase the risk of medication errors and other mistakes. At that point, the incident is no longer just an IT problem. It becomes a threat to patient safety.
Which healthcare laws can be triggered by one cyber incident?
A single cyber incident can set off multiple legal duties at the same time.
Under HIPAA, a breach of unsecured PHI can trigger the Privacy Rule, the Security Rule, and the Breach Notification Rule. That can include notice to affected individuals and to HHS within 60 days.
The same incident may also trigger CIRCIA reporting to CISA, state breach notification laws, 42 CFR Part 2, and the FTC Health Breach Notification Rule for some health apps or vendors that fall outside HIPAA’s scope.
How should hospitals prepare for cyber-related care disruptions?
Hospitals need to treat cybersecurity as part of enterprise risk management and put clinical continuity near the top of the list.
That means building and testing downtime plans before trouble hits. Those plans should cover paper-based or alternate workflows for core systems such as EHRs, labs, and pharmacies. Teams should also spell out which patient safety risks call for diversion or escalation, then check data integrity before bringing systems back to normal use.
Censinet RiskOps™ can help streamline risk assessments and documentation across clinical applications, medical devices, and supply chains.
Related Blog Posts
- One in Three Hospitals Confirm Cyber Incidents Directly Impacted Patient Care in Benchmark Findings
- From breach to bedside: cyber risk is now a patient safety crisis.
- Cybersecurity Benchmark Study Links Cyber Incidents to Direct Patient Safety Concerns
- How Healthcare Organizations Lost Access to Patient Records for 15 Hours - And What Happens Next
