How FDA Cybersecurity Guidance Impacts Access Control
Post Summary
- Key Regulation: Section 524B of the FD&C Act (effective March 29, 2023) applies to "cyber devices" and mandates security measures like authentication, role-based access control (RBAC), and multi-factor authentication (MFA).
- Third-Party Software Risks: Manufacturers must secure third-party components (Software of Unknown Pedigree or SOUP) and provide a Software Bill of Materials (SBOM) to identify vulnerabilities.
- Compliance Challenges: Issues like hardcoded credentials, weak RBAC, and legacy systems can delay FDA approvals or lead to regulatory penalties.
- Lifecycle Security: The FDA requires ongoing security measures, including postmarket monitoring, secure updates, and incident recovery protocols.
- Documentation: Premarket submissions must include threat models, testing evidence, and architecture views to demonstrate compliance.
The stakes are high: healthcare breaches averaged $9.8M per incident in 2024, with attacks on medical devices rising sharply. Manufacturers must implement robust access controls and governance systems to meet FDA standards and protect patients.
Webinar: Master Medical Device Cybersecurity: Avoid FDA Delays
sbb-itb-535baee
Challenges in Meeting FDA Access Control Requirements
Complying with FDA cybersecurity standards isn’t just about checking boxes - it’s about uncovering and addressing critical medical device security risks that could jeopardize patient safety and lead to regulatory consequences. Below, we’ll dive into some of the key issues that make access control compliance so challenging.
Common Access Control Weaknesses in Third-Party Software
Third-party software often comes with built-in security flaws that can be exploited. One major issue is the use of hardcoded credentials, where fixed usernames and passwords are embedded directly in the code, making them easy targets for attackers. On top of that, many third-party tools lack multi-factor authentication (MFA), relying instead on single-factor logins that offer little protection against stolen credentials.
Another weak point is the insufficient implementation of role-based access control (RBAC). When third-party software doesn’t enforce strict user roles, individuals with limited permissions might gain access to sensitive operations or patient data. This is a critical issue, especially considering that remote code execution and privilege escalation attacks on medical devices surged by 437% in 2023 [1]. Many of these attacks were traced back to vulnerabilities in third-party components, emphasizing the FDA's requirement for stringent access control measures across the entire software supply chain.
Regulatory Risks of Poor Access Control
Inadequate access controls don’t just compromise security - they also expose manufacturers to regulatory penalties. For example, under Section 524B of the FD&C Act, manufacturers are required to submit a Software Bill of Materials (SBOM) and show that they actively manage vulnerabilities. If a third-party component contains unpatched authentication flaws, it can delay premarket submissions or prompt the FDA to request additional information, slowing down a product's path to market.
Once a product is released, the stakes get even higher. Starting February 2, 2026, the Quality Management System Regulation (QMSR) mandates that manufacturers integrate cybersecurity requirements into their purchasing specifications, aligning with ISO 13485 Clause 7.4. Any failure in third-party access control could then be classified as a quality system deficiency. This is particularly concerning because a single weak component can compromise the security of the entire system, escalating regulatory scrutiny and potential penalties.
How Third-Party Components Add System-Level Risk
Even a single vulnerable third-party component can compromise an otherwise secure device. For instance, a medical device with strong proprietary firmware could still be at risk if it connects to a third-party Bluetooth module or cloud API with poor access controls [1].
Legacy devices, which can remain in clinical use for as long as 15 years, often run outdated and unpatched third-party software. Without compensating controls like network segmentation, these devices can serve as entry points for attackers into hospital systems. A stark example of this was the 2024 Change Healthcare breach, which exposed data from over 192 million individuals and disrupted U.S. healthcare operations for months [1].
Adding to the complexity is the concept of "Nth-party risk", highlighted in the 2026 MITRE framework. This refers to risks introduced not just by a manufacturer’s direct vendors but also by those vendors’ subcontractors [1]. These cascading risks make it clear why the FDA stresses the need for thorough evaluation of third-party components. Manufacturers must take responsibility for risks that extend beyond the components they can directly inspect or control.
FDA's Specific Requirements for Authentication and Access Control
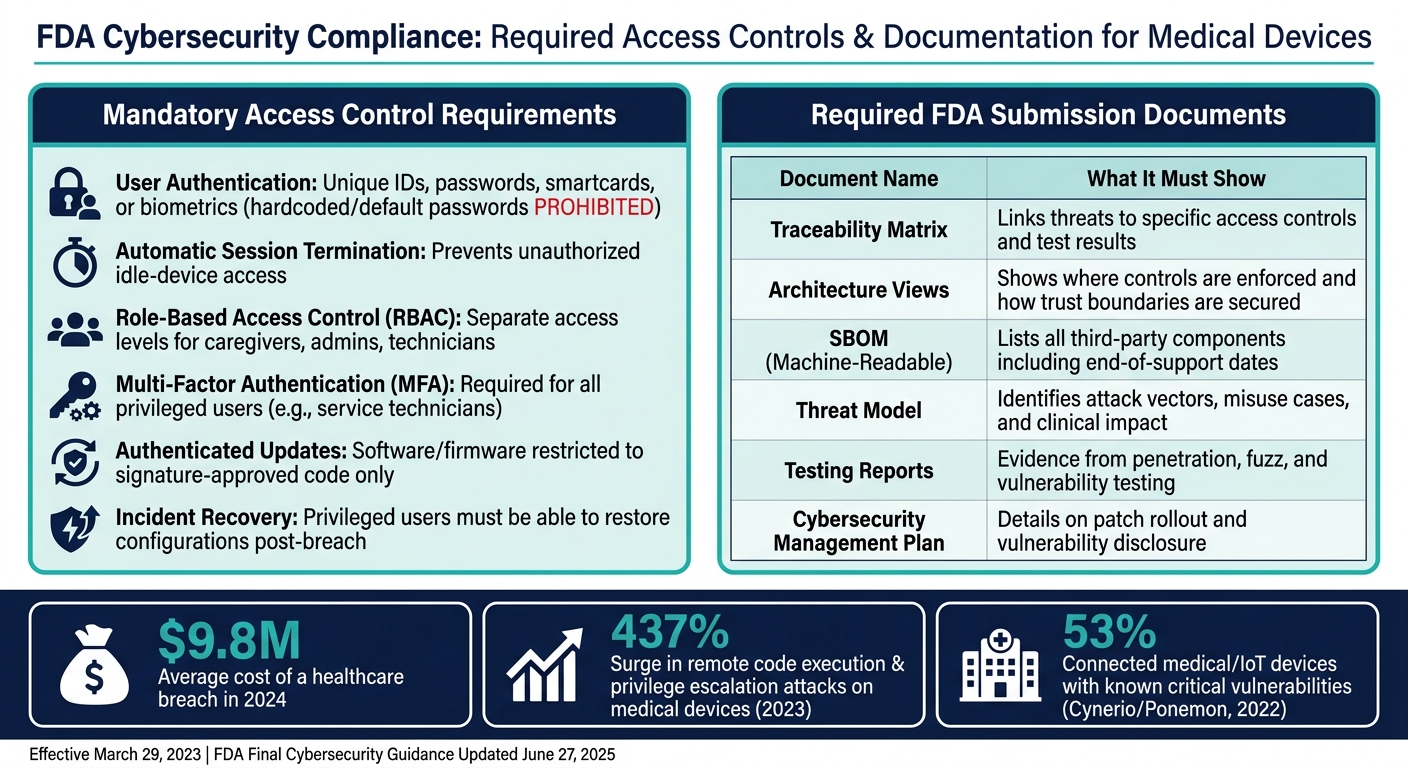
FDA Cybersecurity Compliance: Required Access Controls & Documentation for Medical Devices
The FDA has laid out clear access control standards, covering everything from secure login protocols to recovery after security incidents. Understanding these guidelines is crucial for avoiding delays during premarket reviews.
"The extent to which security controls are needed will depend on the device's intended use, the presence and intent of its electronic data interfaces, its intended environment of use, the type of cybersecurity vulnerabilities present, the likelihood the vulnerability will be exploited... and the probable risk of patient harm." - FDA [2]
Applying Secure Product Development Framework (SPDF) Principles to Access Control
The FDA emphasizes a lifecycle approach to cybersecurity, rooted in a Secure Product Development Framework (SPDF) that integrates with the Quality Management System (QMS) [3]. For access control, traceability is non-negotiable. Manufacturers must link threats, like unauthorized therapy adjustments, to specific security measures, such as authentication methods, and provide evidence that these measures are effective [3].
Access control isn't limited to the medical device itself. The FDA expects it to cover the entire system, including mobile apps, cloud platforms, APIs, update servers, and connection protocols like Wi-Fi, Bluetooth Low Energy (BLE), USB, and NFC [3].
"Reviewers want to know where controls live and what stops compromise from crossing boundaries." - Blue Goat Cyber [3]
The FDA outlines several essential controls for manufacturers to implement:
- User authentication: IDs, passwords, smartcards, or biometrics, with hardcoded or default passwords strictly prohibited [2].
- Automatic session termination: Prevents unauthorized access when devices are idle.
- Role-based access control (RBAC): Differentiates access levels for caregivers, administrators, and other users.
- Multi-factor authentication (MFA): Required for privileged users, such as service technicians [2].
These controls must be thoroughly documented in premarket submissions.
Access Control Documentation for Premarket Submissions
On June 27, 2025, the FDA finalized its guidance on medical device cybersecurity, replacing the September 2023 version and addressing Section 524B of the FD&C Act [4][5]. Premarket submissions must include detailed documentation to justify the chosen security measures.
"Premarket submissions... should justify the security controls chosen for their devices." - FDA [2]
Manufacturers are required to provide:
- Architecture views, including "Multi-Patient Harm Views" that demonstrate how access controls limit widespread risks.
- A threat model that covers the entire system, identifying attack vectors and linking them to clinical risks [6].
- A Software Bill of Materials (SBOM) in a machine-readable format (e.g., SPDX or CycloneDX) [3].
- Testing evidence, such as penetration testing, fuzz testing, and static/dynamic code analysis, to prove the effectiveness of access controls under real-world conditions [6].
The table below summarizes the required documentation and its purpose:
| Required Documentation | What It Must Show |
|---|---|
| Traceability Matrix | Links identified threats to specific access controls and test results [3] |
| Architecture Views | Demonstrates where controls are enforced and how trust boundaries are secured [6] |
| SBOM | Lists all third-party components, including end-of-support dates [6] |
| Threat Model | Identifies attack vectors, misuse cases, and their clinical impact [6] |
| Testing Reports | Evidence from penetration, fuzz, and vulnerability testing [6] |
| Cybersecurity Management Plan | Details on patch rollout and vulnerability disclosure processes [6] |
The FDA takes a broad view of what constitutes a "cyber device." Any device with a USB or serial port is considered internet-capable and must comply with Section 524B requirements [6].
Maintaining Access Control After Market Release
Meeting FDA requirements doesn't end with premarket approval. Under Section 524B, manufacturers must sustain a robust postmarket program to monitor, address, and resolve vulnerabilities throughout the device's lifecycle [3]. This operational commitment reinforces the SPDF principles established during development.
Devices must also include mechanisms to detect, log, and timestamp security events. Even in the event of a security breach, critical functionality must remain operational [2]. For access control, privileged users must be able to restore device configurations following a cybersecurity incident [2]. Additionally, software and firmware updates - such as operating system patches - must be authenticated and restricted to verified, signature-approved code [2].
These ongoing measures ensure that access control remains effective, safeguarding patient safety and device integrity over time.
Building FDA-Compliant Access Control for Third-Party Software
Creating access control mechanisms that meet FDA standards requires a methodical, risk-based approach to design. Let’s break down the key steps to achieve this.
Designing Access Control Based on Risk
Start by mapping out every access point in your system - whether it’s local consoles, web interfaces, mobile apps, APIs, or cloud dashboards. For each access point, consider three critical factors: who connects (e.g., clinicians, biomedical engineers, vendor support), what they can access (e.g., therapy settings, firmware, PHI, logs), and how vulnerable that access point is to potential misuse.
Once identified, rank these access points based on their potential impact on patient safety in a worst-case scenario. For example, an internet-facing vendor portal with the ability to modify device configurations is far riskier than a reporting dashboard that only provides read-only data. High-risk access points should have robust controls in place, such as:
- MFA (Multi-Factor Authentication) for administrative and vendor accounts.
- Role-Based Access Control (RBAC) tailored to clinical roles (e.g., nurse, physician, IT admin).
- Just-in-Time (JIT) Access for sensitive sessions, such as vendor support. For instance, a vendor account might use a time-limited SSH tunnel - active for two hours, fully logged, and automatically revoked after the session ends.
Documenting these risk assessments is crucial, as they must align with FDA premarket submission criteria and broader healthcare third-party risk management standards.
The next step is to address authentication, a critical layer of access control.
Strengthening Authentication Across the Device Stack
Weak or default credentials are a common vulnerability in connected medical devices. A 2022 study by Cynerio and the Ponemon Institute revealed that 53% of connected medical and IoT devices have known critical vulnerabilities, many tied to poor authentication practices. Fixing this requires a layered approach across the device ecosystem.
At the user level, shared accounts for safety-critical actions are unacceptable under FDA guidance. Instead, each user should have a unique account. For shared workflows, implement badge-based single sign-on (SSO) to ensure accountability. For remote or administrative access, integrate with enterprise identity providers using protocols like SAML 2.0 or OAuth 2.0/OIDC. This allows hospitals to enforce their own password and session policies while requiring MFA for sensitive accounts.
For device-to-service communication, secure connections with mutual TLS (mTLS), using per-device certificates stored in secure hardware. Replace hard-coded credentials or shared API keys with token-based authentication, ensuring tokens have documented rotation schedules. If legacy third-party components are involved, isolate them using network segmentation and enforce strong boundary authentication.
Testing Access Controls Through Verification and Validation
Access controls must be tested rigorously to ensure they function as intended. This includes evaluating both normal usage and potential misuse scenarios.
- Penetration testing ensures that authentication mechanisms cannot be bypassed externally.
- Threat modeling, using frameworks like STRIDE, identifies high-risk access paths and ensures third-party components don’t introduce privilege escalation risks.
- Software composition analysis (SCA) helps detect vulnerabilities in authentication libraries before submission to the FDA.
Testing should also include abuse cases, such as scenarios involving compromised vendor credentials or insider threats attempting to escalate privileges. These tests validate whether safeguards like MFA, RBAC, and JIT controls effectively minimize potential harm.
Finally, document all testing evidence - whether from fuzz testing, static code analysis, or dynamic testing - and map it to the access control requirements identified in your threat model. This documentation is essential for meeting FDA cybersecurity compliance standards.
Managing Access Control Governance in Healthcare Organizations
The FDA's cybersecurity guidance emphasizes the importance of maintaining strong governance to ensure vendor access aligns with regulatory standards. Effective access control for devices must go hand-in-hand with well-defined vendor governance policies.
Setting Governance Policies for Third-Party Access
A solid governance framework should clearly outline who is granted access, under what conditions, via which approved channels, and how access is revoked once a contract ends. To minimize risks, apply least-privilege principles and implement just-in-time (JIT) access for vendor accounts. This approach avoids leaving persistent administrative credentials active outside of scheduled maintenance periods. Policies should also specify approved remote access methods - such as VPNs with device certificates or zero-trust remote support brokers - while explicitly banning consumer-grade remote desktop tools.
These vendor policies must be integrated into the organization’s Quality Management System (QMS), IT change management processes, and clinical engineering workflows. For instance, if a vendor needs to update firmware on a medical device like an infusion pump, the request should follow a documented protocol rather than relying on informal communication, such as email.
Contracts and Business Associate Agreements (BAAs) should mandate security measures like multi-factor authentication (MFA), unique account credentials, a software bill of materials (SBOM), and timely incident notifications (within 24–48 hours). Additionally, include clauses granting the right to audit vendor compliance.
Such policies establish a foundation for continuous and rigorous oversight of vendor activities.
Monitoring Vendors and Managing Risk on an Ongoing Basis
Ongoing monitoring is critical to managing vendor-related risks effectively. High-risk vendors - especially those with privileged access to medical devices or protected health information (PHI) - should undergo formal risk reassessments at least once a year. For vendors with elevated access, reassessments should occur every six months. Unscheduled reassessments are necessary after events like security incidents, major software updates, discovery of critical vulnerabilities, or patterns of unusual access.
Vendor and privileged sessions should be routed through monitored channels, such as Privileged Access Management (PAM) solutions or secure remote access gateways, to ensure detailed session logs are generated. Feeding these logs into a Security Information and Event Management (SIEM) system allows for anomaly detection, such as access attempts outside normal hours or repeated MFA failures. Quarterly access certifications help update vendor risk ratings in the enterprise risk register and trigger Corrective and Preventive Actions (CAPAs) when systemic issues are identified.
Incorporating these findings into the organization’s Cybersecurity Management Plan (CMP) ensures alignment with FDA lifecycle cybersecurity risk management expectations. This creates a feedback loop that strengthens the overall governance process.
Tools like Censinet RiskOps™ can simplify and automate these monitoring tasks, ensuring consistent oversight.
Using Censinet to Manage Third-Party Risk
Relying solely on manual governance methods can leave gaps, exposing healthcare organizations to significant risks. A 2022 study by the Ponemon Institute revealed that 89% of healthcare organizations experienced an average of 43 third-party-related incidents in the prior year. Over a two-year period, 55% reported at least one cyberattack tied to a third-party vendor that disrupted patient care.
Censinet RiskOps™ offers a tailored solution for healthcare organizations. The platform conducts comprehensive risk assessments, focusing on areas like authentication, remote access controls, and access logging for vendors of medical devices and clinical software. With the support of Censinet AI™, vendors can complete security questionnaires in seconds. Automated tools summarize evidence and generate risk reports, while human oversight ensures critical decisions are carefully evaluated.
For ongoing governance, Censinet RiskOps™ tracks changes in vendor risk profiles, flags when reassessments are needed, and benchmarks vendor access control practices against industry standards. This seamless integration of procurement and governance workflows enables healthcare organizations to manage large vendor portfolios effectively. By identifying high-risk vendors early, organizations can proactively address potential issues before they escalate into contractual disputes or security incidents.
Conclusion: Aligning Access Control With FDA Cybersecurity Guidance
The FDA's cybersecurity guidance emphasizes the need for proactive, lifecycle-wide access control measures. According to Section 524B of the FD&C Act and the FDA's June 2025 Final Cybersecurity Guidance, security must span the total product lifecycle (TPLC) - it's not just a box to check during submission. This means implementing authentication controls, designing with least-privilege principles, and managing third-party access from development through the entire clinical use of the device.
The stakes are high. Persistent vulnerabilities affect more than half of connected medical devices, and healthcare data breaches cost an average of $9.8 million in 2024 [1]. Weak access controls, especially in third-party components, are a major factor in these costly breaches.
To meet FDA expectations, manufacturers need to address risks across the entire device stack. This includes eliminating hardcoded credentials, enforcing multi-factor authentication (MFA) for privileged access, maintaining an up-to-date software bill of materials (SBOM), and regularly updating threat models as new vulnerabilities arise. Governance policies, vendor agreements, and continuous monitoring must work together seamlessly - because a single weak link can compromise the entire system.
Tools like Censinet RiskOps™ provide a way to streamline and structure this process. By transforming what might otherwise be a chaotic, manual effort into an organized, auditable program, these solutions help healthcare organizations go beyond regulatory compliance. The ultimate goal is ensuring that the devices patients rely on remain secure throughout their entire lifecycle.
FAQs
Does my device count as a "cyber device" under Section 524B?
Your device falls under the definition of a "cyber device" as outlined in Section 524B of the FD&C Act if it meets these three criteria: it includes software, can connect to the internet, and has features that could be exposed to cybersecurity threats. These standards are in place to ensure that devices with potential vulnerabilities adhere to FDA cybersecurity guidelines.
What access controls does the FDA expect for vendor and service accounts?
The FDA mandates stringent access controls for vendor and service accounts to protect medical devices and connected systems. These measures include the use of unique credentials, multi-factor authentication (MFA), and layered authorization. Together, they help prevent unauthorized access and ensure secure system management.
How do I prove RBAC and MFA work in an FDA premarket submission?
To showcase Role-Based Access Control (RBAC) and Multi-Factor Authentication (MFA) as part of an FDA premarket submission, you'll need to provide detailed documentation that highlights their design, implementation, and effectiveness. Here's what to include:
- Architecture Diagrams: Present clear, annotated diagrams illustrating how RBAC and MFA are integrated into your system. Highlight user roles, authentication workflows, and interactions between components.
- Access Control Matrices: Provide a matrix that maps user roles to specific permissions. This should demonstrate how access is restricted based on roles and how sensitive functions are protected.
- Test Results: Include results from functional and security testing to prove that RBAC and MFA operate as intended. For RBAC, show tests that verify role-specific access restrictions. For MFA, provide evidence of successful multi-factor authentication under different scenarios.
- Risk Mapping: Create a table or document that links identified risks to specific controls. For example, tie the risk of unauthorized access to the implementation of RBAC and MFA mechanisms.
- Validation Through Testing: Document test cases that validate the controls. This might include penetration testing for MFA robustness or attempts to bypass RBAC restrictions.
- Ongoing Monitoring Procedures: Outline how you will monitor and maintain RBAC and MFA compliance over time. This could include periodic audits, automated alerts for anomalies, and updates to address emerging threats.
By providing comprehensive and well-organized evidence, you can demonstrate compliance with FDA cybersecurity guidance while ensuring that your system is secure and reliable.

